


The Uncomfortable Truth About Brain Health Guidelines
Every few years, a major health organization releases a list of things you should do to prevent dementia, and every time, the public treats it like gospel. The American Heart Association just published their latest—10 factors for brain resilience—and while some of it is solid, the fundamental premise contains a dangerous assumption that neuroscience moved past a decade ago.
Here’s what they won’t tell you outright: most dementia is not preventable through lifestyle alone, and pretending otherwise sets patients up for guilt when cognitive decline happens anyway. But that doesn’t mean these factors are useless—it means we need to be honest about what they actually do and why.
What the AHA Got Right (And What They’re Still Not Saying)
The AHA’s framework focuses on cardiovascular health as brain health, which is scientifically sound. Your brain uses 20% of your body’s oxygen despite being only 2% of your mass. When blood flow deteriorates, neurons die. Period.
Their ten factors break down into categories: blood pressure control, cholesterol management, blood sugar regulation, physical activity, diet quality, body weight, smoking cessation, sleep quality, social connection, and cognitive engagement. The AHA published this framework in Stroke journal based on decades of cardiovascular research showing that vascular dementia—cognitive decline from stroke and small vessel disease—is largely modifiable.
But here’s the critical nuance: vascular dementia represents only 15-20% of all dementia cases. Alzheimer’s disease, which accounts for 60-70% of cases, has a much more complex relationship with these lifestyle factors. The mechanism isn’t just blood flow—it’s about amyloid-beta plaques, tau tangles, neuroinflammation, and genetic factors we can’t lifestyle our way out of.
The Biology They’re Not Explaining Clearly
Let me walk you through what actually happens in your brain when these factors go wrong, because understanding the mechanism changes how you think about prevention.
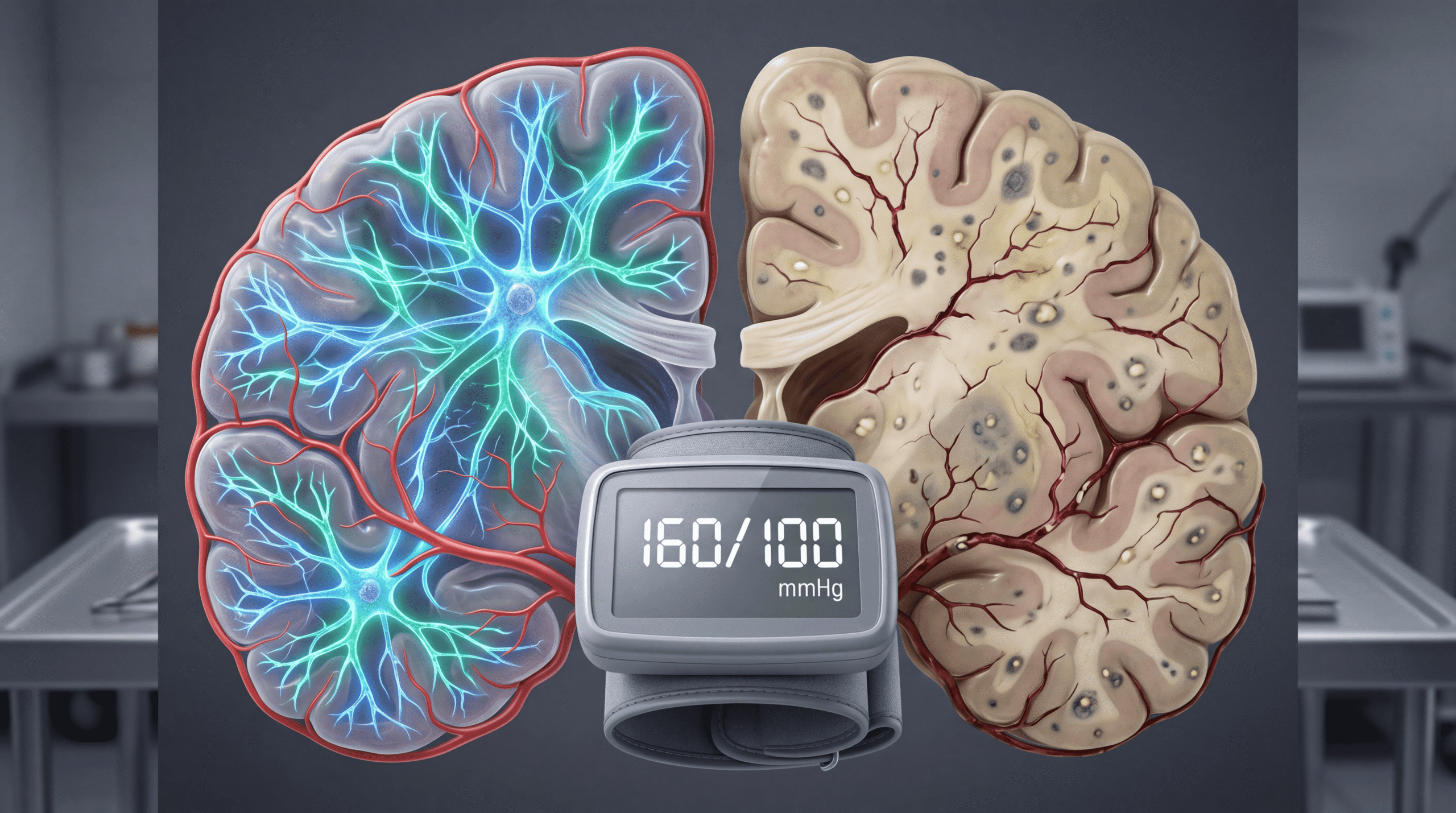
Blood pressure matters because chronic hypertension damages the blood-brain barrier. This barrier is a specialized layer of cells that keeps toxins out of your brain tissue. When it breaks down from sustained high pressure, inflammatory proteins leak in and trigger microglial activation—your brain’s immune cells go haywire and start destroying synapses they should be protecting. NIH research from 2023 showed this process begins in your 40s, decades before symptoms appear.
Sleep deprivation prevents glymphatic clearance. Your brain has a waste removal system that activates primarily during deep sleep, flushing out metabolic debris including amyloid-beta proteins. When you consistently sleep less than 7 hours, these proteins accumulate. One night of poor sleep increases brain amyloid by 5%. Chronic sleep restriction creates a compounding debt your brain cannot metabolize away during occasional good nights.
Physical inactivity reduces BDNF production. Brain-derived neurotrophic factor is essentially fertilizer for neurons—it promotes new synaptic connections and neurogenesis in the hippocampus. Exercise, particularly aerobic activity that raises your heart rate to 60-80% of maximum for 30+ minutes, triggers BDNF release. Sedentary individuals have measurably smaller hippocampal volumes by age 60, according to imaging studies published in NeuroImage.
The Three Habits That Actively Accelerate Cognitive Decline
Most articles tell you what to do. I’m going to tell you what actually destroys brain tissue faster than normal aging, because avoiding harm matters more than optimizing wellness.
1. Chronic high blood sugar variability. Notice I didn’t say “diabetes”—I said variability. Your brain runs on glucose, but wild swings in blood sugar trigger a process called glycation, where sugar molecules bind to proteins and form advanced glycation end products (AGEs). These literally stiffen blood vessels in your brain. A 2024 study tracking 5,000 adults found that glycemic variability predicted dementia risk better than average blood sugar levels.
2. Social isolation combined with hearing loss. This is a synergistic disaster. Hearing loss forces your brain to reallocate cognitive resources to basic auditory processing, stealing capacity from memory and executive function. Social isolation removes the cognitive stimulation that builds reserve. Together, they create a 60% higher dementia risk than either alone, per the Lancet Commission on Dementia Prevention.
3. Unmanaged sleep apnea. Every apneic episode—where you stop breathing—causes a micro-surge in blood pressure and deprives your brain of oxygen. Do this 30 times an hour for years, and you create permanent white matter damage visible on MRI. The scary part? Most people with sleep apnea don’t know they have it because they’re unconscious when it happens. If your partner says you snore loudly and sometimes stop breathing, get a sleep study. This is not optional.
What the Media Consistently Gets Wrong About Brain Health
Every time research like the AHA’s framework gets published, headlines scream “10 Ways to Prevent Dementia!” This is scientifically irresponsible for three reasons.
First, it conflates risk reduction with prevention. Reducing risk by 30-40% still means 60-70% of risk remains, much of it genetic and unavoidable. APOE4 carriers have up to 15 times higher Alzheimer’s risk regardless of lifestyle. Telling people they can prevent dementia through behavior sets them up for self-blame when genetics pulls the trigger anyway.
Second, it ignores the lag time between intervention and outcome. Most lifestyle studies follow people for 10-20 years and find associations, not causation. We don’t have randomized trials proving that starting exercise at 60 prevents dementia at 80 because such trials would take 20 years and cost billions. What we have is observational data showing people who exercised in their 60s had less dementia in their 80s—but we don’t know if the exercise caused it or if healthier brains made exercise more likely.
Third, it oversimplifies multifactorial disease. Dementia isn’t one thing. Calling it “brain health” lumps together vascular dementia, Alzheimer’s disease, Lewy body dementia, and frontotemporal dementia—diseases with different mechanisms requiring different approaches. The AHA’s framework works beautifully for vascular dementia. For Alzheimer’s? The evidence is much weaker.
The Cognitive Reserve Theory Nobody Explains Properly
Here’s the concept that makes sense of all this: cognitive reserve. Your brain can accumulate pathology—plaques, tangles, vascular damage—without showing symptoms if you’ve built enough reserve through mental stimulation, education, and complex work.
Autopsies of high-functioning elderly people often reveal brains riddled with Alzheimer’s pathology that never caused clinical dementia. Their brains built redundant neural networks that compensated for damage. The National Institute on Aging has documented this phenomenon in multiple longitudinal studies.
This is why education level predicts dementia risk independent of lifestyle. It’s not that educated people make better choices (though they might)—it’s that intellectual challenge throughout life builds a neurological buffer. You can’t go back and get more education at 70, but you can engage in cognitively demanding activities: learning languages, playing musical instruments, strategic games, complex social interaction.
What You Should Actually Do (The Evidence-Based Version)
Let me give you the protocol I actually recommend to patients based on mechanism, not just epidemiological association.
Blood pressure control is non-negotiable. Target below 130/80 starting in your 40s. The brain damage from hypertension is irreversible, so prevention is everything. If lifestyle changes don’t achieve this in 3 months, medication is appropriate. This is not a failure—it’s acknowledging biology.
Prioritize sleep architecture over duration. Seven hours of deep, restorative sleep beats nine hours of fragmented sleep. If you wake up frequently, snore, or feel unrefreshed after adequate time in bed, investigate sleep apnea, restless legs, or anxiety. Treating the underlying disorder matters more than sleep hygiene tips.
Exercise for BDNF, not weight loss. The brain benefits of exercise are independent of weight changes. Thirty minutes of activity that makes you slightly breathless—brisk walking, cycling, swimming—five times weekly produces measurable increases in hippocampal volume within 6 months. This is one of the few interventions with MRI-proven structural brain changes.
Manage hearing loss aggressively. Get your hearing tested at 60 if not sooner. If you need hearing aids, wear them consistently. The cognitive load of compensating for hearing loss is substantial and measurable. Modern hearing aids are sophisticated medical devices, not vanity items to avoid.
Social connection requires depth, not breadth. You don’t need a large network. You need meaningful relationships that require complex social cognition—understanding others’ perspectives, navigating disagreements, maintaining long-term commitments. Weekly phone calls with close friends may be more protective than monthly large gatherings with acquaintances.
The One Number That Matters More Than All Others
If I could monitor only one biomarker for brain health, it would be blood pressure variability between visits. Not average blood pressure—variability. Wild swings in systolic pressure from appointment to appointment predict dementia better than consistently elevated pressure.
This suggests that vascular stability matters more than absolute values. Ask your doctor to track your blood pressure trend over years, not just whether you’re “controlled” at each visit. The American Heart Association now recognizes visit-to-visit variability as an independent risk factor for both stroke and dementia.
Why Genetics Isn’t Destiny (But It’s Not Irrelevant)
APOE4 is the strongest genetic risk factor for Alzheimer’s disease. Having one copy triples your risk; two copies increase it 8-12 fold. But here’s what gets lost: most APOE4 carriers never develop Alzheimer’s, and 40% of Alzheimer’s patients don’t carry APOE4 at all.
Knowing your APOE status doesn’t change what you should do—the interventions are the same. But it might change your urgency in implementing them. Some patients want to know; others prefer not to live with that knowledge. Both choices are valid. What’s not valid is genetic testing companies selling APOE testing without proper counseling about what the results mean and don’t mean.
The Brutal Truth About Supplements and Brain Health
I’m going to save you money: no supplement has proven efficacy in preventing dementia in rigorous trials. Not omega-3s, not vitamin E, not ginkgo biloba, not B vitamins. Large randomized controlled trials have tested all of them. They failed.
The COSMOS-Mind trial published in 2023 tested a multivitamin and found a small benefit, but it was modest and the formulation was specific. The over-the-counter brain supplements you see advertised have no evidence behind them—they’re marketing, not medicine.
If you’re deficient in a vitamin, correcting that deficiency is important. But taking megadoses of vitamins when you’re not deficient doesn’t create a super-brain. It creates expensive urine.
What Actually Builds Cognitive Reserve After 60
Contrary to popular belief, novelty matters more than difficulty. Your brain grows when forced to create new neural pathways, not when refining existing ones. This means:
Learning a new language provides more cognitive benefit than becoming more fluent in one you already speak. Taking up an instrument as an adult challenges your brain more than practicing one you’ve played for decades. Traveling to unfamiliar places where you must navigate uncertainty creates more neuroplasticity than routine vacations to favorite spots.
The common factor is discomfort—the feeling that you’re not good at something yet. That struggle is neurogenesis in action. Most people avoid it. The people who age cognitively well seek it out deliberately.
The Intervention Window Nobody Talks About
Here’s the timing issue that matters: most lifestyle interventions show benefit when started in midlife, not late life. Starting aggressive cardiovascular risk reduction at 45 prevents dementia at 75. Starting it at 70 prevents stroke but may not move the dementia needle much.
This is because the pathological process of Alzheimer’s disease begins 15-20 years before symptoms appear. By the time you have mild cognitive impairment, amyloid plaques have been accumulating for decades. We’re trying to prevent that accumulation, not reverse it once it’s extensive.
Does this mean starting healthy habits at 70 is pointless? Absolutely not. It means the benefits are different—maintaining function, preventing vascular dementia, improving quality of life—but may not prevent Alzheimer’s disease that’s already in process.
What You Should Actually Do Today
Schedule three appointments: primary care for blood pressure and blood sugar assessment, audiology for baseline hearing test, and sleep medicine if you snore or wake unrefreshed. These are the modifiable factors with the strongest mechanistic evidence.
Then commit to one cognitively challenging activity that makes you uncomfortable: sign up for language classes, join a complex strategy game group, take up an instrument. The goal isn’t mastery—it’s sustained novelty that forces your brain to build new networks.
Brain health isn’t about perfection in ten categories. It’s about aggressive management of vascular risk factors, consistent cognitive challenge, and honest acknowledgment that some risk remains beyond your control. You can’t prevent all dementia, but you can maximize your odds and maintain function longer when decline does occur. That’s not failure—that’s working with biology instead of against it.


