



The Medical Establishment’s Comfortable Lie
For decades, physicians have handed asthma patients prednisone prescriptions with the reassuring phrase “just a short course.” Here’s what they don’t tell you: there’s no such thing as a harmless corticosteroid burst. Every single dose triggers a cascade of metabolic disruptions that your body remembers long after the pills are gone.
I’ve watched colleagues prescribe oral corticosteroids (OCS) like candy—three, four, five courses per year—while patients develop the classic steroid toxicity syndrome: moon face, buffalo hump, paper-thin skin that tears at the slightest touch. Then everyone acts surprised when the bone density scan comes back showing osteoporosis in a 42-year-old.
The Biological Reality No One Explains
Oral corticosteroids work by mimicking cortisol and binding to glucocorticoid receptors throughout your entire body—not just your lungs. This triggers a massive suppression of nuclear factor kappa B (NF-κB), the master switch for inflammatory gene transcription. Sounds great until you realize this same mechanism simultaneously:
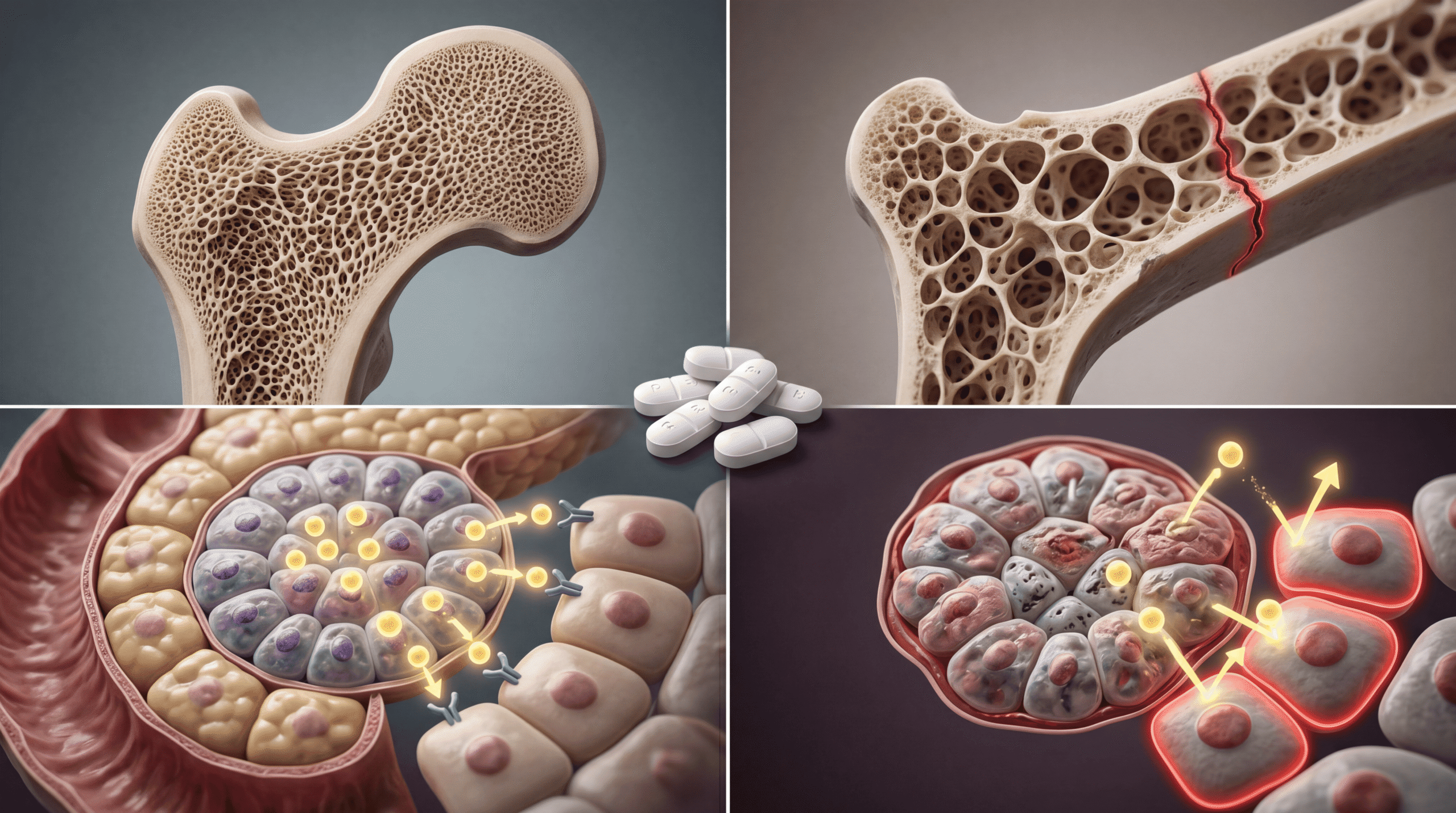
Shuts down osteoblast activity (the cells that build bone) while ramping up osteoclast function (the cells that dissolve bone). The NIH documented that cumulative OCS doses above 1,000mg lifetime significantly increase fracture risk—and most severe asthma patients blow past that threshold in two years.
Induces insulin resistance by interfering with GLUT4 glucose transporter expression in muscle and adipose tissue. This isn’t theoretical: Lancet Respiratory Medicine research found that just three OCS courses annually increases type 2 diabetes risk by 20% over five years.
Suppresses your hypothalamic-pituitary-adrenal (HPA) axis, meaning your adrenal glands forget how to make their own cortisol. Patients develop secondary adrenal insufficiency, then can’t mount a stress response during surgery or severe illness—a potentially fatal complication conveniently buried in the fine print.
What The Media Got Wrong
Healthcare journalists love the narrative of “lifesaving asthma medications” without understanding the pharmacology. They report on emergency room visits prevented by OCS without mentioning the emergency room visits caused by OCS complications five years later.
The mainstream coverage completely misses that oral and inhaled corticosteroids are not equivalent. Inhaled corticosteroids (ICS) deliver medication directly to airway tissue with minimal systemic absorption. Oral corticosteroids flood your entire bloodstream, hitting every organ system.
When you see headlines celebrating how “affordable steroids save lives in developing countries,” they’re ignoring that these same patients develop premature cardiovascular disease, avascular necrosis of the hip, and psychiatric disorders at rates that dwarf their wealthy-nation counterparts who have access to biologic therapies.
The Prescribing Culture That Kills Slowly
Here’s the dirty secret: OCS prescriptions persist because they’re easy. A $4 generic prednisone prescription makes the wheezing stop right now. The patient feels better within hours. The doctor looks like a hero.
Meanwhile, optimizing inhaled controller therapy takes weeks of patient education, technique assessment, and medication titration. Prescribing biologics requires insurance authorization, specialty pharmacy coordination, and injection training. Pulmonologists are incentivized to reach for the quick fix.
I’ve reviewed charts where patients received 8-10 OCS courses annually for “severe asthma”—except nobody bothered to check if they were actually using their inhaler correctly. Studies in the American Journal of Respiratory and Critical Care Medicine show that up to 70% of patients demonstrate critical errors in inhaler technique, rendering their controller medications useless.
The Biologic Revolution Your Insurance Doesn’t Want You To Know About
The treatment landscape has fundamentally changed, but prescribing patterns haven’t caught up. We now have five distinct classes of biologic medications targeting specific inflammatory pathways in severe asthma:
Anti-IgE therapy (omalizumab) blocks the allergic cascade at its source by binding immunoglobulin E before it triggers mast cell degranulation. Anti-IL-5 agents (mepolizumab, reslizumab, benralizumab) deplete eosinophils, the white blood cells driving inflammation in eosinophilic asthma phenotypes. Anti-IL-4Rα (dupilumab) blocks both IL-4 and IL-13 signaling, disrupting the Type 2 inflammatory pathway that characterizes most moderate-to-severe asthma.
These aren’t experimental—they’re FDA-approved, guideline-recommended, and dramatically reduce OCS dependence. New England Journal of Medicine trials demonstrated that dupilumab reduced OCS requirements by 70% in steroid-dependent asthma patients while simultaneously improving lung function and quality of life.
The problem? A year of biologic therapy costs $30,000-40,000 versus $50 for a year’s supply of prednisone. Insurance companies deny authorization, citing “medical necessity” requirements that essentially mandate patients fail every cheaper option first—meaning they must document steroid toxicity before accessing safer alternatives.
What You Should Actually Do
If you’re taking more than two OCS courses per year, your asthma is not controlled and your treatment plan is failing. Demand the following from your physician:
Step 1: Inhaler technique assessment. Schedule an appointment specifically to demonstrate your inhaler use while someone watches and corrects errors. Poor technique is the leading cause of “treatment-resistant” asthma. Request a peak flow meter and learn your personal best values.
Step 2: Phenotype your asthma. Ask for blood eosinophil count, total IgE level, and fractional exhaled nitric oxide (FeNO) testing. These biomarkers identify which patients benefit from specific biologic therapies. This isn’t optional anymore—it’s standard of care per NHLBI 2020 asthma guidelines.
Step 3: Demand biologic consideration. If you meet criteria (moderate-to-severe asthma, elevated biomarkers, frequent exacerbations despite maximal inhaled therapy), your doctor should be submitting prior authorization. If they claim “insurance won’t cover it,” that’s often physician laziness—specialty pharmacies exist specifically to handle authorization appeals.
Step 4: Protect your bones NOW. If you’ve had significant OCS exposure (cumulative dose >1,000mg or frequent courses), get a DEXA scan for bone density. Start calcium 1,200mg and vitamin D 2,000 IU daily. Discuss bisphosphonate therapy with your doctor if osteoporosis is documented.
Step 5: Monitor for metabolic damage. Annual hemoglobin A1C to screen for diabetes, ophthalmology exams for cataracts, and cardiovascular risk assessment should be mandatory for anyone with chronic OCS exposure. These complications are preventable if caught early.
The Global Health Catastrophe
The OCS problem is exponentially worse in low-resource settings. In East Africa, where I’ve consulted on respiratory programs, generic prednisone is often the only available asthma medication beyond short-acting bronchodilators.
Patients in Nairobi or Mombasa face impossible choices: use oral steroids and develop complications, or don’t use them and die during severe exacerbations. The cold chain infrastructure required for biologic distribution doesn’t exist in rural Kenya. Even inhaled corticosteroids are unaffordable for most families.
International health organizations pat themselves on the back for providing “essential medications” while ignoring that we’re essentially exporting a slower form of morbidity. WHO estimates that 80% of asthma deaths occur in low- and middle-income countries—not because the disease is more severe, but because treatment options create their own pathology.
Why This Matters More Than Headlines Suggest
The corticosteroid crisis represents everything broken about modern medicine: we have superior treatments but economic and systemic barriers prevent their use. Physicians continue harmful prescribing patterns out of inertia. Insurance companies prioritize short-term costs over long-term outcomes. Patients suffer complications that were entirely preventable.
This isn’t about demonizing a medication class—oral corticosteroids saved countless lives before alternatives existed, and they still have a role in true emergency situations. But the routine, repeated, cavalier prescribing for poorly controlled asthma is medical malpractice hiding behind decades of tradition.
The human cost is staggering: every prednisone prescription issued to avoid the administrative hassle of optimizing controller therapy or pursuing biologic authorization represents a conscious choice to prioritize physician convenience over patient welfare.
The Hard Truth About Modern Asthma Care
If your asthma treatment plan hasn’t been updated in the last three years, you’re receiving obsolete care. The field has transformed, but most primary care physicians and even some pulmonologists are still practicing 1990s medicine in 2025.
The acceptable use of oral corticosteroids in asthma should be: severe exacerbations requiring emergency intervention (where the immediate mortality risk justifies the toxicity), and short-term bridges while awaiting biologic therapy initiation (measured in weeks, not months or years).
Everything else is lazy medicine, and you deserve better. Your bones deserve better. Your pancreas deserves better. Your immune system deserves better.
Demand that your physician treat your asthma like it’s 2025, not 1985—because the difference between those two approaches is the difference between living well and merely surviving with progressive, preventable complications.
Here’s your power move: Walk into your next appointment with your cumulative corticosteroid dose calculated (multiply each course by the daily dose and duration), your biomarker levels printed, and one question ready: “Why am I not on a biologic yet?” Watch how fast the conversation changes when you demonstrate you understand the medicine better than they assumed.


