


The headlines are calling it a “holy grail” for sleep apnea, but let me tell you what they’re not saying: this new pill won’t cure your sleep apnea, won’t work for most severe cases, and certainly won’t match the efficacy of properly used CPAP therapy. After thirty years treating sleep disorders, I’m watching another pharmaceutical “breakthrough” get wildly oversold to desperate patients who already struggle with one of medicine’s most undertreated conditions.
What This Drug Actually Does (And Doesn’t Do)
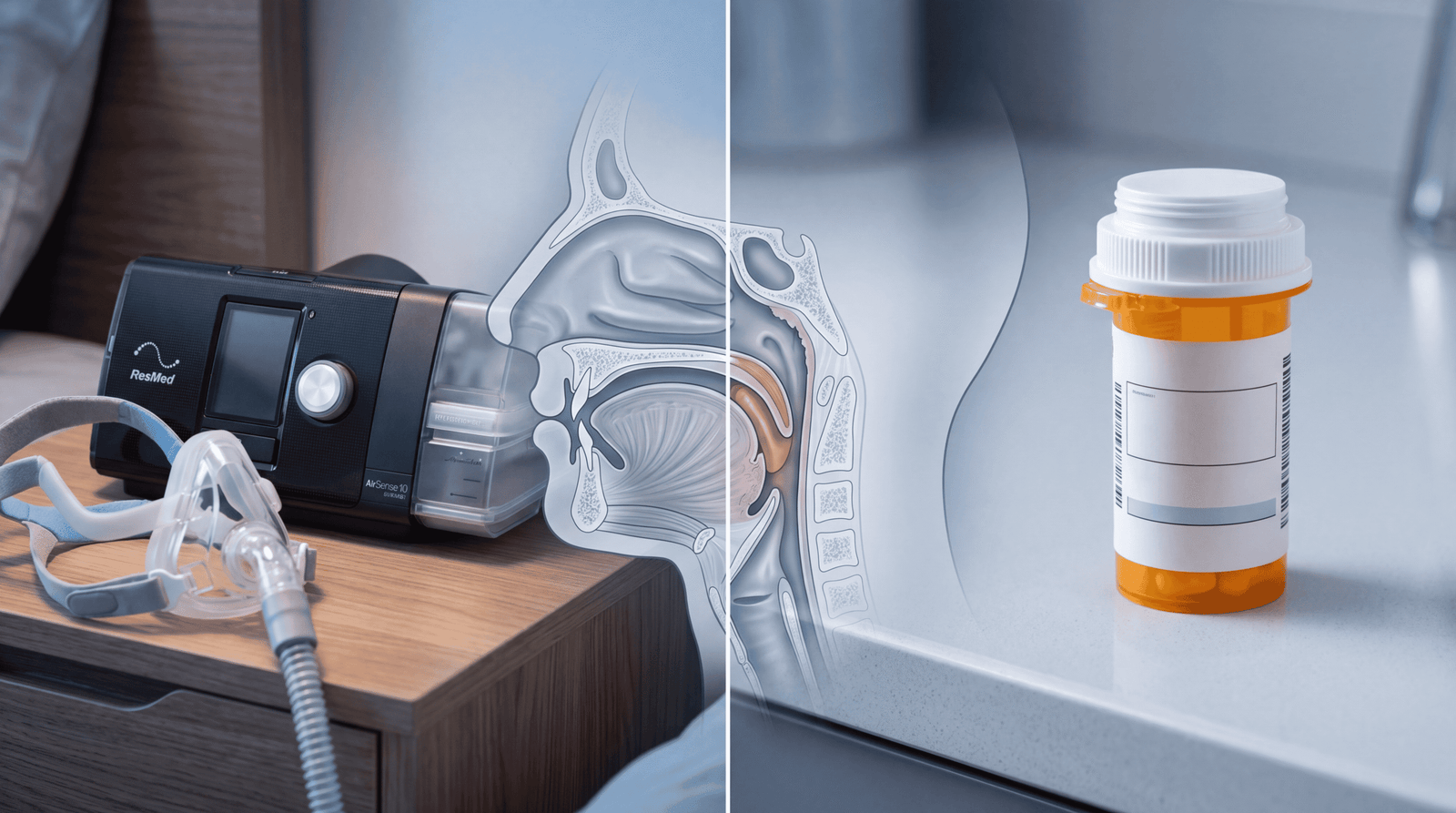
The medication generating buzz is a combination of aroxybutynin and atomoxetine, which works by targeting the hypoglossal nerve that controls tongue muscle tone during sleep. When your airway collapses during sleep apnea, it’s often because the muscles at the base of your tongue relax too much. This drug keeps those muscles slightly more engaged.
Here’s the mechanism: atomoxetine is a norepinephrine reuptake inhibitor that increases upper airway muscle tone, while aroxybutynin blocks muscarinic receptors that would otherwise cause muscle relaxation. Together, they reduce the apnea-hypopnea index (AHI)—the number of breathing disruptions per hour—by approximately 50-60% in clinical trials according to data published in the New England Journal of Medicine.
That sounds impressive until you understand what CPAP does: it reduces AHI by 85-95% in compliant users. We’re comparing a 50% reduction with a near-complete elimination of breathing events. The math isn’t even close.
The CPAP Reality Check No One Wants to Hear
Here’s what drives me crazy about this narrative: the problem with CPAP isn’t that it doesn’t work—it’s that patients won’t use it. Studies from the American Academy of Sleep Medicine consistently show that CPAP adherence hovers around 30-40% at one year. When patients actually wear the device for at least four hours per night, it’s extraordinarily effective.
CPAP delivers positive airway pressure that physically prevents your airway from collapsing. It’s mechanical, immediate, and doesn’t depend on drug metabolism, liver function, or drug interactions. The moment you put on the mask, your oxygen saturation improves, your blood pressure stabilizes, and your brain gets the restorative sleep it desperately needs.
The new pill works through neurotransmitter manipulation, which means it’s subject to tolerance, side effects, and the variability of individual pharmacokinetics. Some patients metabolize these drugs rapidly and get minimal benefit. Others experience intolerable side effects like dry mouth, insomnia (ironic, isn’t it?), increased heart rate, and urinary retention.
Who This Drug Might Actually Help
I’m not entirely dismissive of this medication—there’s a legitimate role for it, but it’s much narrower than the marketing suggests. The clinical trials focused on patients with mild to moderate obstructive sleep apnea (OSA), defined as an AHI of 15-50 events per hour. For these patients who absolutely refuse CPAP or cannot tolerate it despite proper mask fitting and pressure adjustments, this pill represents a genuine alternative.
The World Health Organization estimates that over 936 million adults worldwide have mild to severe OSA. But here’s the critical distinction: severe sleep apnea (AHI greater than 50) wasn’t well-represented in the drug trials, and these patients face significantly higher cardiovascular risk. For someone with an AHI of 70 who stops breathing more than once per minute, a 50% reduction still leaves them with dangerous levels of oxygen desaturation.
The drug also appears more effective in patients with lower body mass index. The mechanism makes sense—if anatomical obstruction from obesity is the primary driver, no amount of neurotransmitter tweaking will overcome the physics of tissue mass narrowing your airway. According to research from the National Institutes of Health, every 10% increase in body weight increases OSA risk by six-fold, and these patients need mechanical support that drugs simply cannot provide.
What The Media Got Wrong
The “holy grail” framing fundamentally misrepresents how we should think about sleep apnea treatment. This isn’t a cure. It’s not even disease-modifying. The moment you stop taking the pill, your muscle tone returns to baseline and your apnea returns to full severity. You’re trading a nightly mechanical device for a daily medication with systemic effects and ongoing costs.
News coverage consistently fails to report the actual reduction in cardiovascular events, which is what we actually care about. Sleep apnea isn’t dangerous because it makes you tired—it’s dangerous because repetitive oxygen desaturation causes endothelial dysfunction, increases sympathetic nervous system activation, and drives hypertension, atrial fibrillation, and stroke risk. The Lancet published data showing that untreated severe OSA increases all-cause mortality by 46%.
We don’t yet have long-term outcome data showing this pill prevents heart attacks and strokes with the same efficacy as CPAP. We have surrogate markers like AHI reduction and oxygen saturation improvement, but those aren’t the same as “will I live longer and healthier.” CPAP has decades of cardiovascular outcome data. This pill has months.
The other massive omission: cost and insurance coverage. CPAP machines are durable medical equipment covered by most insurance with a one-time expense. This medication will require daily dosing indefinitely. At current estimates, we’re looking at $200-300 per month without insurance. Over ten years, that’s $24,000-36,000 compared to a $1,500 CPAP machine. The pharmaceutical industry loves chronic medication, but your wallet might not.
The Real Comparison: Mechanism vs. Mechanism
Let’s talk biology. Your upper airway contains more than 20 different muscle groups, all coordinated by complex neural signaling during sleep. Obstructive sleep apnea occurs when these muscles relax excessively during REM sleep, when skeletal muscle tone naturally decreases as part of normal sleep architecture.
CPAP bypasses this entire neuromuscular system by creating a pneumatic splint—positive pressure that physically prevents collapse regardless of muscle tone. It works in every sleep stage, isn’t affected by alcohol or sedatives, and doesn’t require any physiological response from your body. It’s elegant mechanical engineering solving a mechanical problem.
The pill approach tries to chemically override the natural relaxation that’s supposed to happen during sleep. You’re essentially keeping your upper airway muscles in a semi-contracted state all night through sustained norepinephrine signaling. This isn’t restoring normal physiology—it’s creating a pharmacologically altered state to compensate for anatomical predisposition.
There’s also the issue of sleep architecture itself. Studies using polysomnography show that CPAP improves sleep quality by reducing arousal frequency and allowing deeper, more restorative sleep stages. We don’t yet know if chronic norepinergic stimulation during sleep affects REM latency, sleep spindle density, or slow-wave sleep percentage—all markers of sleep quality that matter for cognitive function and metabolic health. The Journal of Clinical Sleep Medicine has documented that sleep fragmentation, independent of oxygen desaturation, drives many of the metabolic consequences of OSA.
What You Should Actually Do
If you have diagnosed obstructive sleep apnea, your first-line treatment should still be CPAP or an oral appliance, period. The evidence base is overwhelming, the efficacy is unmatched, and the long-term safety profile is excellent. If you’ve tried CPAP and struggled, here’s what you need to do before jumping to medication:
Get a proper mask fitting. Most CPAP failures are actually mask failures—wrong size, wrong style, air leaks causing discomfort. A sleep center should offer multiple mask types: nasal pillows, nasal masks, and full-face masks. Try them all. I’ve had patients go through five different masks before finding one they’d actually wear.
Optimize your pressure settings. Auto-titrating CPAP machines adjust pressure throughout the night based on airflow resistance. If you’re on a fixed-pressure machine and feeling like you’re suffocating or struggling to exhale, you need a pressure adjustment. This isn’t optional—it’s essential.
Address your weight if BMI is above 30. I’m not saying this to be unkind—I’m saying it because a 10% weight loss can reduce AHI by 26% according to Mayo Clinic data. For some patients, this alone eliminates the need for any device or medication. Combine weight loss with CPAP and you might eventually graduate to a dental appliance or no treatment at all.
Now, if you’ve genuinely exhausted these options—proper mask fitting, pressure optimization, positional therapy, weight management—and still cannot tolerate CPAP, this new medication may be worth discussing with your sleep physician. But understand you’re accepting a less effective treatment with unknown long-term consequences and ongoing costs. That’s a trade-off, not a miracle.
The Hidden Danger of “Easy” Solutions
My biggest concern with this drug isn’t the medication itself—it’s what it represents psychologically. We’ve created a medical culture where patients expect pills to solve problems that require behavioral change or tolerance of mild discomfort. CPAP isn’t fun. Neither is wearing glasses, taking blood pressure medication, or using a continuous glucose monitor. But we do these things because the alternative is disease progression and early death.
Sleep apnea kills by inches—gradual endothelial damage, progressive left ventricular hypertrophy, incremental cognitive decline from repetitive hypoxemia. You don’t feel your coronary arteries developing atherosclerotic plaques. You don’t notice your hippocampus shrinking from chronic sleep fragmentation. By the time you have symptoms—the heart attack, the stroke, the dementia—the damage is done.
The pharmaceutical narrative suggests you can avoid all that unpleasantness with a simple pill. But a 50% reduction in AHI might not be enough to prevent cardiovascular consequences. We’re seeing the same pattern we saw with diabetes medications that lowered glucose without reducing heart attacks, or blood pressure medications that hit numerical targets without improving outcomes. Surrogate markers aren’t the same as the outcomes that actually matter.
What Comes Next
This drug will likely receive FDA approval—the phase 3 trial data shows statistically significant AHI reduction with manageable side effects in selected patients. It will be marketed aggressively because there’s enormous profit potential in converting a one-time device purchase into a daily medication. Insurance companies will initially cover it, then develop prior authorization requirements mandating CPAP failure before approval.
In five years, we’ll have real-world effectiveness data, long-term cardiovascular outcomes, and better understanding of which patient phenotypes respond best. We might discover that certain genetic polymorphisms affecting norepinephrine receptor density predict drug response. We might find that combination therapy—medication plus CPAP at lower pressures—offers the best adherence and outcomes.
But today, in 2026, with the data we currently have, calling this a “holy grail” is pharmaceutical marketing dressed up as medical journalism. It’s a useful addition to our therapeutic toolkit, particularly for patients with mild disease who refuse first-line therapy. It’s not a revolution.
Your Action Plan
Get a sleep study if you snore loudly, wake up gasping, or feel unrefreshed despite adequate time in bed—these are signs of OSA that predict cardiovascular risk. If diagnosed, commit to a genuine CPAP trial with proper support, not a half-hearted two-week attempt with an ill-fitting mask. Give it three months with optimization before declaring failure. Your brain, your heart, and your longevity will thank you for tolerating temporary discomfort in exchange for effective treatment that actually prevents the diseases that kill us.


