


Here’s what nobody tells you about allergy medications: most people are using them completely wrong, which is why they report that ‘nothing works anymore.’ The problem isn’t drug resistance — your immune system doesn’t develop tolerance to antihistamines the way bacteria resist antibiotics. The real issue is that you’re treating symptoms after the inflammatory cascade has already begun, like trying to bail water out of a boat instead of plugging the hole.
I’ve been practicing internal medicine for over two decades, and the single most common mistake I see is patients taking antihistamines after they start sneezing. By then, your mast cells have already degranulated, releasing not just histamine but also leukotrienes, prostaglandins, and cytokines — a whole inflammatory soup that a simple antihistamine can’t touch. This is why you feel like your medication ‘isn’t working’ when you actually need a completely different approach.
The Mechanism Most Doctors Don’t Explain (But Should)
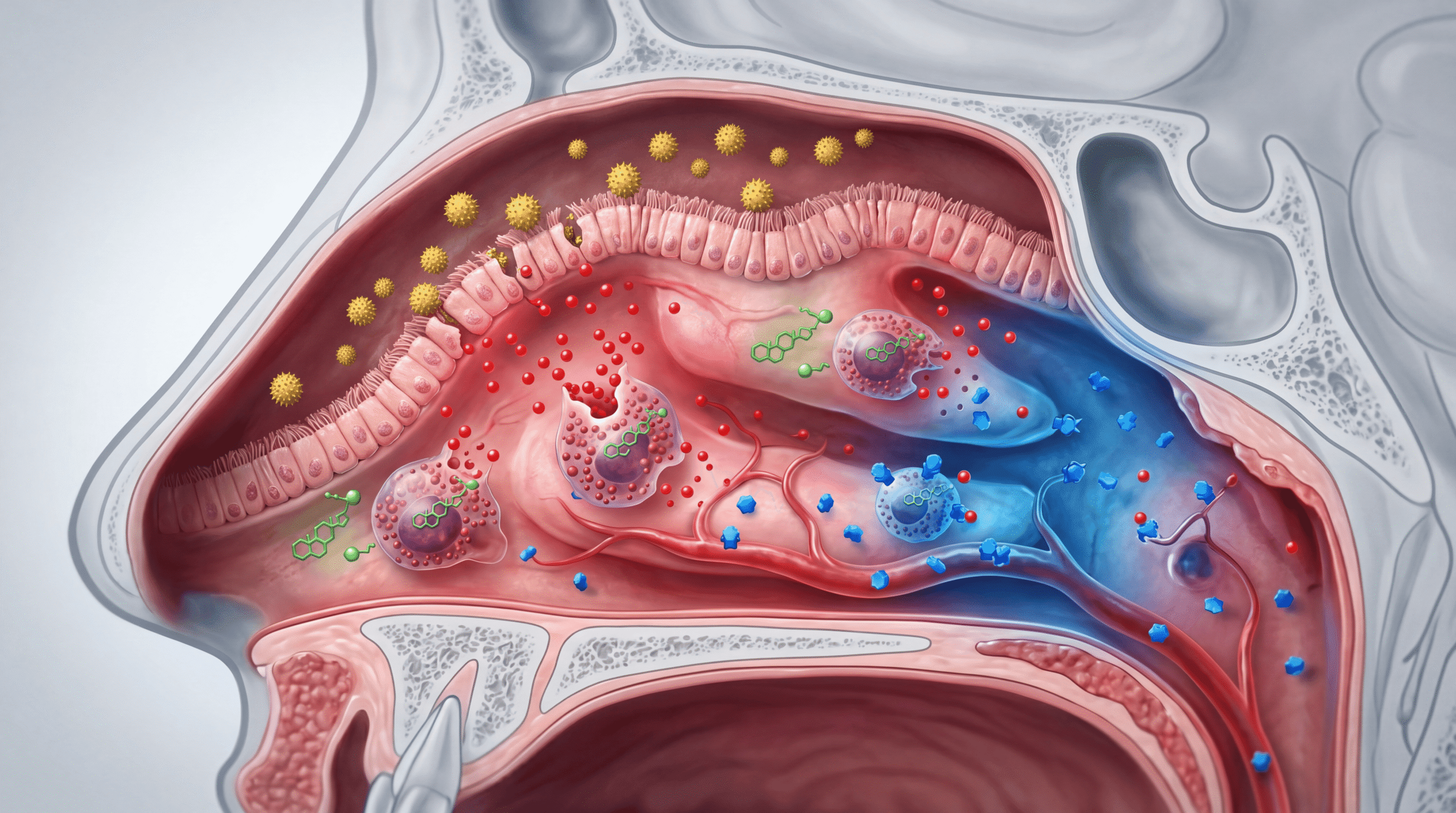
When pollen lands on your nasal mucosa, it doesn’t immediately cause symptoms. First, it binds to IgE antibodies on mast cells. This triggers degranulation — the mast cell literally explodes, releasing preformed mediators stored in granules. Histamine is just one of dozens of inflammatory chemicals released, which is why blocking histamine alone often feels inadequate.
The histamine binds to H1 receptors on blood vessels, causing vasodilation (that stuffy feeling) and increased vascular permeability (why your nose runs). It also stimulates nerve endings (the itch) and triggers mucus production. Second-generation antihistamines like cetirizine (Zyrtec), fexofenadine (Allegra), and levocetirizine (Xyzal) block these H1 receptors peripherally without crossing the blood-brain barrier significantly, which is why they cause less sedation than older drugs like diphenhydramine (Benadryl).
But here’s the critical part: histamine represents only about 15-20% of the total inflammatory response in allergic rhinitis. The rest comes from leukotrienes, prostaglandins, and late-phase inflammatory cells like eosinophils that arrive hours after the initial exposure. This is why you can take an antihistamine and still feel congested and miserable.
What The Media Got Wrong About ‘Non-Drowsy’ Antihistamines
Magazine articles love to rank allergy medications by ‘drowsiness potential,’ as if that’s the main differentiator. This completely misses the point. The real question is whether you’re using a medication that addresses your specific inflammatory pathway, not just blocking one receptor.
Yes, cetirizine causes more sedation than fexofenadine in clinical trials — about 10-15% of users report drowsiness versus 2-3% with fexofenadine, according to comparative studies in the Journal of Allergy and Clinical Immunology. But that same study showed cetirizine was more effective at reducing total symptom scores, probably because it has modest anti-leukotriene activity in addition to H1 blockade.
The media also perpetuates the myth that you should ‘try different antihistamines to see what works.’ This is backwards. If an antihistamine isn’t working, you probably don’t need a different antihistamine — you need a medication that targets a different part of the inflammatory cascade entirely. That’s where intranasal corticosteroids come in.
Why Nasal Steroids Beat Antihistamines (And Nobody Tells You)
Fluticasone propionate (Flonase), mometasone (Nasonex), and triamcinolone (Nasacort) work through a completely different mechanism. These glucocorticoids inhibit phospholipase A2, the enzyme that produces arachidonic acid, which is the precursor to both prostaglandins and leukotrienes. They also reduce the number of mast cells, eosinophils, and other inflammatory cells in your nasal mucosa over time.
This is why intranasal steroids take 1-2 weeks to reach full effect — they’re changing the cellular composition of your nasal lining, not just blocking receptors. Multiple meta-analyses in Cochrane Reviews show intranasal corticosteroids are more effective than oral antihistamines for nasal congestion, the symptom patients find most bothersome.
The safety profile is excellent. Despite the word ‘steroid,’ these medications act locally with minimal systemic absorption. You won’t get the side effects associated with oral prednisone — no weight gain, no mood changes, no adrenal suppression at recommended doses. The most common side effect is minor nosebleeds from mucosal drying, which you can prevent by aiming the spray toward the outer wall of your nostril (away from the septum) and using a saline rinse afterward.
The Xyzal Marketing Hype: Prescription Strength Doesn’t Mean Better
Levocetirizine (Xyzal) is marketed as ‘prescription strength’ now available OTC, which sounds impressive until you understand what it actually is. Xyzal is the R-enantiomer of cetirizine — essentially, it’s half of the Zyrtec molecule. Cetirizine is a racemic mixture (50% R-enantiomer, 50% S-enantiomer), and the R-form is the active one.
In theory, using only the active enantiomer should provide equal efficacy at half the dose with fewer side effects. In practice, clinical trials show minimal difference. A 5mg dose of levocetirizine performs similarly to 10mg cetirizine in head-to-head studies. The ‘prescription strength’ language is marketing — both drugs were originally prescription-only before going OTC.
The claim that Xyzal is safe for children as young as 6 months is technically true, but here’s the context doctors know: antihistamines in infants under 2 years should be used with extreme caution and only under pediatric supervision, regardless of FDA approval. Infants metabolize drugs differently, and there’s insufficient long-term safety data. I never recommend chronic antihistamine use in this age group without compelling indication.
Azelastine: The Nasal Spray Most People Should Try First
Azelastine (Astepro, Astelin) is an antihistamine nasal spray that was prescription-only until recently. Unlike oral antihistamines, it delivers high local concentrations directly to the nasal mucosa where the allergic reaction is happening. It starts working in 15-30 minutes because it doesn’t need to be absorbed, distributed through bloodstream, and then diffuse to target tissue — it’s already there.
The pharmacology is interesting: azelastine blocks H1 receptors like oral antihistamines, but it also stabilizes mast cells (preventing degranulation) and inhibits the synthesis of leukotrienes and prostaglandins. This multi-mechanism approach makes it more effective than you’d expect from the ‘antihistamine’ label. Studies in Annals of Allergy, Asthma & Immunology show it works as well as intranasal steroids for many patients.
The main downside is taste. About 20% of users report a bitter aftertaste (I’m one of them). This happens because the medication drips down the back of your throat. To minimize this, spray while bending your head forward slightly and don’t sniff forcefully — let the medication stay in your nose. Some patients use a strong mint afterward to mask the taste.
The Combination Strategy That Actually Works
Here’s what I prescribe for patients with moderate to severe allergic rhinitis, and it’s based on understanding that allergic inflammation has multiple pathways that need simultaneous blockade: intranasal corticosteroid once daily plus azelastine nasal spray twice daily. This combination addresses the inflammatory cytokines, leukotrienes, prostaglandins, and histamine.
You can use them sequentially (azelastine first, wait 5 minutes, then the steroid) or try Dymista, which is a fixed combination of both in one bottle. The advantage of Dymista is convenience and probably better compliance. The disadvantage is cost — combination products are always more expensive than buying components separately, and insurance coverage varies.
For rapid symptom relief on top of this foundation, an oral antihistamine can help with breakthrough itching and eye symptoms. Fexofenadine is my first choice because it has the lowest sedation risk and no cardiac effects (older antihistamines like terfenadine were pulled from the market for causing QT prolongation). Take it consistently during allergy season, not just when symptoms flare.
The Eye Drop Strategy Nobody Mentions
Allergic conjunctivitis is miserable, and most people either tough it out or use general ‘redness relief’ drops that contain vasoconstrictors like tetrahydrozoline. These are terrible long-term solutions because they cause rebound hyperemia — when they wear off, your eyes get even redder than before, so you use more drops, creating a dependency cycle.
Antihistamine eye drops like ketotifen (Zaditor, Alaway) work by blocking H1 receptors in the conjunctiva and also stabilizing mast cells. They start working in minutes and last 8-12 hours. Unlike oral antihistamines, which have to reach the eye via systemic circulation, topical drops deliver high local concentrations with minimal side effects. They don’t cause rebound redness and are safe for long-term use.
If ketotifen doesn’t fully control symptoms, olopatadine (Pataday) is more potent but usually requires a prescription. For severe allergic conjunctivitis, I sometimes add a corticosteroid eye drop like loteprednol short-term (under 2 weeks), but never use steroid eye drops without ophthalmologic supervision — prolonged use can cause glaucoma and cataracts.
Why Your Allergies Get Worse Every Year (It’s Not Your Imagination)
Patients frequently tell me their allergies are worse than they used to be, and they’re right. Climate data from the NIH shows pollen seasons are starting earlier and lasting longer due to rising temperatures, with total pollen loads increasing by 20% over the past two decades. Ragweed season alone has extended by nearly 3 weeks in most of North America.
There’s also an immunological phenomenon called ‘priming.’ Repeated allergen exposure over a season increases the sensitivity of your mast cells and the number of IgE antibodies, so the same pollen load triggers a bigger response later in the season. This is why starting medications before symptoms begin is so effective — you prevent the priming effect from developing.
The other factor is the ‘hygiene hypothesis’ playing out at a population level. Reduced childhood exposure to diverse microbes and parasites may skew the immune system toward Th2 responses (allergy) instead of Th1 responses (cellular immunity). This is contentious and incomplete, but it’s consistent with rising allergy prevalence in industrialized countries.
The Medications That Don’t Work (Despite Being Everywhere)
Let’s talk about what’s ineffective. Oral decongestants like pseudoephedrine and phenylephrine have minimal benefit for allergic rhinitis, especially phenylephrine, which the FDA recently concluded has no evidence of efficacy at standard oral doses. Pseudoephedrine works modestly but causes tachycardia, hypertension, insomnia, and urinary retention, especially in older adults. It’s behind the pharmacy counter because it’s a methamphetamine precursor, not because it’s particularly effective.
Nasal decongestant sprays like oxymetazoline (Afrin) work instantly but cause severe rebound congestion if used more than 3 consecutive days. I’ve seen patients dependent on Afrin for years, with rhinitis medicamentosa so severe they can’t breathe without it. Breaking this cycle requires stopping the spray (which is miserable for 5-7 days) while using intranasal steroids and sometimes a short oral prednisone burst.
Homeopathic allergy treatments have no plausible mechanism and no evidence of efficacy beyond placebo in rigorous trials. Same with most herbal supplements marketed for allergies. Butterbur extract has some limited data but was associated with liver toxicity. Quercetin is a mast cell stabilizer in vitro but has poor oral bioavailability and inconsistent human data.
What You Should Actually Do (The Protocol I Use Myself)
I have ragweed allergy, so I practice what I preach. Here’s my personal protocol, which I also recommend to patients: Start fluticasone nasal spray 2 weeks before ragweed season (early August where I live), use it daily through October. Add azelastine nasal spray on high pollen days or when I have breakthrough congestion. Keep fexofenadine 180mg tablets available for days when I’m doing outdoor activities during peak pollen hours.
I check pollen counts via weather apps or pollen.com, and I adjust medication intensity accordingly. On low pollen days, I might skip the antihistamine. On very high days, I use all three medications. I also use saline nasal rinses (NeilMed sinus rinse) after being outdoors to mechanically remove pollen from my nasal passages before it triggers inflammation.
For patients with severe symptoms despite maximal medical therapy, I discuss allergen immunotherapy — either subcutaneous injections (allergy shots) or sublingual tablets. Immunotherapy gradually desensitizes the immune system by exposing it to increasing allergen doses, shifting the response from IgE-mediated (allergic) to IgG-mediated (tolerant). It takes 3-5 years of treatment but can provide lasting benefit even after stopping, unlike medications which only work while you’re taking them.
The Side Effect Nobody Warns You About
Chronic untreated allergic rhinitis doesn’t just make you miserable — it significantly impairs sleep quality, cognitive function, and productivity. Studies using objective measures like the Psychomotor Vigilance Test show that untreated allergic rhinitis causes performance deficits equivalent to a blood alcohol level of 0.05%, right at the legal driving limit in many countries. This isn’t from antihistamine sedation (which is mild and often resolves with continued use) but from the allergic inflammation itself disrupting sleep architecture.
I see this clinically all the time: patients come in complaining of fatigue, poor concentration, and irritability, assuming these are separate problems. Then we treat their allergies aggressively, and suddenly they feel like a different person. The nasal congestion causes mouth breathing at night, which leads to sleep fragmentation, reduced REM sleep, and daytime impairment. Don’t underestimate the systemic impact of ‘just allergies.’
What The Research Shows About Long-Term Safety
Patients worry about using medications chronically, which is reasonable. The safety data is reassuring: second-generation antihistamines have been used for decades with no evidence of significant long-term adverse effects. A systematic review in Drug Safety covering millions of patient-years of exposure found no increased risk of cardiovascular events, cancer, or other serious outcomes compared to non-users.
Intranasal corticosteroids are similarly safe. Concerns about growth suppression in children have been studied extensively — at standard doses, there’s no clinically significant effect on final adult height. Nasal septal perforation can occur with improper technique (spraying directly at the septum repeatedly), but is rare when used correctly. Systemic absorption is minimal; plasma cortisol levels remain normal.
The real long-term risk is not treating allergies adequately, which is associated with development of asthma (the ‘allergic march’), chronic sinusitis, nasal polyps, and the sleep and cognitive impacts I mentioned. Treat your allergies aggressively early rather than letting inflammation persist for years.
When To Stop Self-Treating And See A Specialist
Most allergic rhinitis can be managed with the OTC strategies I’ve outlined, but some situations require specialist evaluation. See an allergist if you have persistent symptoms despite 4-6 weeks of maximal medical therapy (intranasal steroid plus antihistamine plus nasal antihistamine), if you’re developing asthma symptoms (wheezing, chest tightness, chronic cough), or if you have recurrent sinus infections.
Other red flags: unilateral nasal symptoms (could be structural issue or tumor, not allergy), bloody nasal discharge (needs endoscopy to rule out serious pathology), severe facial pain (sinusitis or other diagnosis), or symptoms that persist year-round without seasonal variation (might be non-allergic rhinitis, which requires different treatment).
Allergists can perform skin testing or specific IgE blood tests to identify your exact allergens, which is useful if you’re considering immunotherapy or need to know what to avoid. They can also prescribe stronger medications like oral leukotriene inhibitors (montelukast) or biologics like omalizumab for severe cases.
The real breakthrough in allergy treatment isn’t a new drug — it’s understanding that inflammation has multiple pathways requiring different interventions, starting treatment before symptoms begin, and staying consistent rather than chasing symptoms after they start. Your immune system is complex, but once you match the right medication to the right mechanism at the right time, allergies become manageable rather than a seasonal nightmare that you just endure.


