



Here’s what your doctor probably didn’t mention when prescribing that Z-pack: a single course of antibiotics can permanently alter your gut microbiome, and new research from isolated indigenous populations proves we’ve been catastrophically wrong about how quickly this happens.
I’m going to challenge something fundamental that medical schools teach. We’ve told patients for decades that antibiotic disruption is “temporary” and your gut “bounces back.” That’s not just incomplete — it’s dangerously misleading.
The Yanomami Discovery That Changed Everything
When researchers studied the Yanomami people of the Amazon — a population with zero previous contact with Western medicine — they found gut microbiome diversity 30-40% higher than the average American. These weren’t subtle differences. We’re talking about entire families of bacteria that simply don’t exist in Western guts anymore.
The shocking part? When researchers returned just two years later after minimal medical intervention (primarily basic antibiotics for acute infections), measurable microbiome changes had already occurred. Not in a generation. Not in a decade. In 24 months.
The Mechanism No One Explains to Patients
Here’s the biology your doctor should have explained before writing that prescription. Your gut contains approximately 100 trillion bacteria — outnumbering your human cells 10 to 1. These aren’t passengers; they’re active participants in everything from serotonin production (90% happens in your gut) to immune system training.
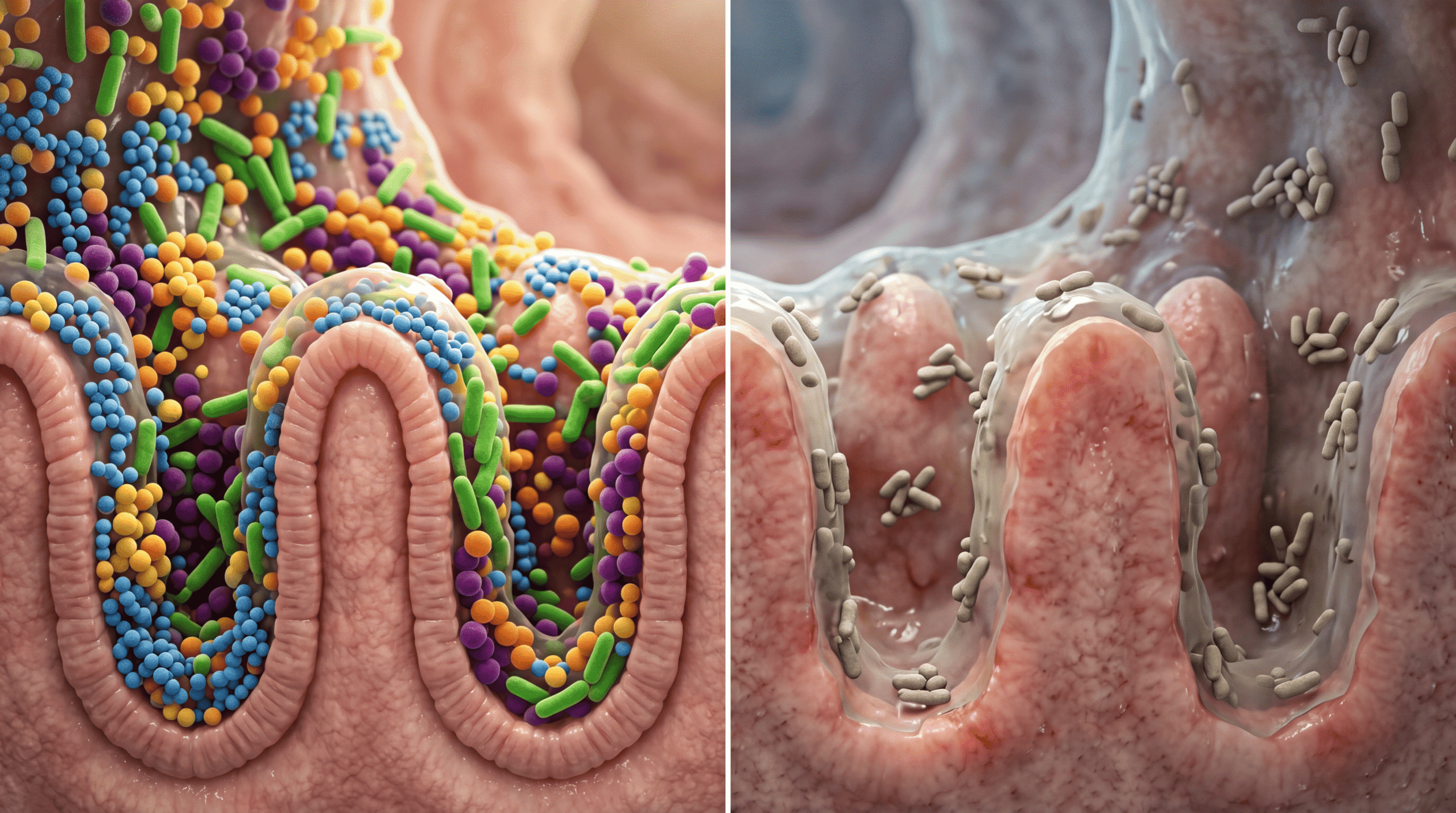
When you take a broad-spectrum antibiotic like amoxicillin or ciprofloxacin, you’re essentially napalming an entire ecosystem. The drug doesn’t discriminate between pathogenic E. coli causing your UTI and beneficial Bifidobacterium that produce short-chain fatty acids protecting your colon lining.
The critical mechanism mainstream medicine ignores: microbiome recovery isn’t just about bacterial count returning to normal. It’s about diversity and functional capacity. Research published in Nature shows that while total bacterial numbers may rebound within weeks, specific keystone species can remain depleted for years or never return.
Why Indigenous Guts Are Microbiome Gold Standards
The Hadza tribe of Tanzania, the Matsés of Peru, and isolated Mongolian populations share something remarkable: bacterial strains that have completely vanished from industrialized populations. These aren’t random bacteria — they’re functional powerhouses.
One example: Prevotella copri, abundant in hunter-gatherer populations, excels at breaking down plant fibers into beneficial metabolites. It’s nearly extinct in Western guts. When researchers at Stanford tried to reintroduce it to Westerners through fecal transplants, it couldn’t establish itself. The ecological niche had been filled by other, less beneficial species.
This is ecological succession in action. Once you lose keystone bacterial species, the gut landscape fundamentally changes. It’s not just about taking a probiotic — the entire ecosystem has shifted to a new, less diverse equilibrium state.
The Antibiotic Cascade Effect
Here’s what actually happens on a cellular level when you take antibiotics, based on metabolomic studies from Cell:
Days 1-3: Broad-spectrum kill-off begins. Both pathogenic and commensal bacteria die en masse. Bacterial metabolites that regulate intestinal permeability drop precipitously.
Days 4-10: Opportunistic species (often less beneficial) rapidly colonize the emptied niches. This is why Clostridioides difficile infections spike post-antibiotic — there’s no competition. Your gut’s immune tolerance shifts because the bacteria that were training your T-cells are gone.
Weeks 2-8: Diversity appears to recover on basic sequencing. This is when doctors tell you you’re “fine.” But functional gene analysis shows critical metabolic pathways remain impaired. Butyrate production (essential for colon cell health) can stay depressed for months to years.
Months 3-12+: In many patients, the microbiome never returns to baseline. Studies tracking individuals for two years post-antibiotic show persistent depletion of specific bacterial genera, particularly those producing anti-inflammatory compounds.
What The Media Consistently Gets Wrong
Every article about probiotics after antibiotics misses the fundamental point: you can’t simply replace what was lost. The commercial probiotic industry has sold us a fiction.
Most over-the-counter probiotics contain 5-10 bacterial strains. Your gut normally houses 500-1000 species. It’s like trying to restore the Amazon rainforest by planting a few houseplants. The math doesn’t work.
Even more problematic: most probiotic strains (Lactobacillus and Bifidobacterium species) are transient colonizers. They pass through your system without establishing permanent residence. That’s not necessarily bad — they can have beneficial effects during transit — but it’s not restoration.
The media also perpetuates the myth that “eating yogurt” fixes antibiotic damage. A single serving of yogurt contains roughly 1 billion CFU (colony-forming units) of bacteria. Your gut contains 100 trillion bacteria. Even if every yogurt bacterium survived and colonized (they don’t), you’re talking about 0.001% replacement.
The PPIs and NSAIDs Connection Nobody Discusses
Antibiotics get all the attention, but proton pump inhibitors (Prilosec, Nexium) and NSAIDs (ibuprofen, naproxen) also significantly alter gut microbiome composition. PPIs reduce stomach acid, allowing bacteria that normally can’t survive gastric pH to colonize the upper GI tract.
Research from Gut (the journal) shows PPI users have markedly different microbiome profiles, with overgrowth of oral bacteria in the intestines — bacteria that have no business being there. This contributes to small intestinal bacterial overgrowth (SIBO) and increases infection risk.
NSAIDs directly damage the intestinal lining, increasing permeability (“leaky gut” isn’t pseudoscience when we’re talking about measurable tight junction disruption). This changes the gut environment, favoring bacteria that thrive in inflammatory conditions over beneficial commensals.
The Hygiene Hypothesis on Steroids
Indigenous populations like the Yanomami teach us something profound about the hygiene hypothesis. We thought it was about exposure to dirt and pathogens training the immune system. It’s actually about continuous bacterial diversity exposure from birth onward.
C-sections, formula feeding, antibiotics in the first year of life, and sanitized environments don’t just reduce pathogen exposure — they prevent the establishment of beneficial bacterial networks. Studies comparing Amish children (low allergy rates) to suburban children (high rates) found the difference wasn’t cleanliness but bacterial diversity transmitted through environmental contact.
When Yanomami infants are born, they’re colonized by their mother’s vaginal and skin bacteria, then continuously exposed to a bacterial-rich environment with no antibacterial soaps, no antibiotics, and constant contact with soil and plants containing diverse microbes. This isn’t romanticizing primitive living — it’s acknowledging we’ve accidentally created a microbially depleted environment.
The Intergenerational Transmission Problem
Here’s the truly disturbing part emerging from recent research: microbiome depletion compounds across generations. When you have reduced microbial diversity and pass a depleted microbiome to your children, they start with less diversity than you had. Their children start with even less.
Mouse studies (which translate surprisingly well to humans in microbiome research) show that four generations of antibiotics and Western diet create irreversible microbiome changes. Even when the great-great-grandchildren of the original mice were given high-fiber diets and no antibiotics, certain bacterial families couldn’t be restored. They were functionally extinct from that mouse lineage.
We don’t have four-generation human studies yet, but we have something arguably more concerning: comparing current Western microbiomes to historical DNA from ancient fecal samples and contemporary isolated populations. We’ve lost entire bacterial phyla in just 100-150 years of industrialization and modern medicine.
The Resistant Starch Gap
Indigenous populations consuming 100-150 grams of fiber daily (versus the American average of 15 grams) aren’t just eating more vegetables. They’re consuming massive amounts of resistant starch — the primary food source for beneficial colon bacteria.
Resistant starch (found in cooked-then-cooled potatoes, green bananas, and certain roots) reaches your colon undigested. Bacteria ferment it into short-chain fatty acids, particularly butyrate. Butyrate is the primary fuel for colonocytes (colon cells) and has powerful anti-inflammatory effects.
Here’s the mechanism most doctors don’t know: butyrate activates T-regulatory cells, suppressing inappropriate immune responses. Low butyrate production is associated with inflammatory bowel disease, colon cancer, and systemic inflammation. When you nuke your butyrate-producing bacteria with antibiotics and don’t feed the remaining bacteria resistant starch, you’ve created a perfect storm for chronic inflammation.
What You Should Actually Do
Before antibiotics: Have a legitimate conversation with your physician about necessity. Viral infections (most upper respiratory infections, bronchitis, many ear infections) don’t benefit from antibiotics. The research is unequivocal, yet 30% of outpatient antibiotic prescriptions in the US are inappropriate. Demand justification.
When antibiotics are necessary: Take them — bacterial infections can be life-threatening. But understand you’re making a calculated trade-off. Use the narrowest-spectrum antibiotic that will work. A targeted antibiotic like penicillin for strep throat causes less collateral damage than azithromycin.
During and after antibiotics: Forget commercial probiotics for a moment. Focus on feeding beneficial bacteria that survived. Increase resistant starch (cooked-then-cooled potatoes and rice, green bananas, oats), fermented foods with live cultures (real sauerkraut, kimchi, kefir — not shelf-stable versions), and soluble fiber (oats, beans, lentils, flax).
If you want to try probiotics, Saccharomyces boulardii (a beneficial yeast) has the strongest evidence for preventing antibiotic-associated diarrhea and C. diff colonization. It’s not affected by antibiotics (it’s not a bacterium) and can protect the gut lining during antibiotic treatment.
Long-term strategy: Diversity is key. Aim for 30+ different plant foods weekly (herbs and spices count). Each plant contains different fibers that feed different bacterial populations. This isn’t about quantity; it’s about variety.
Consider judicious PPI use. If you’ve been on omeprazole for years for mild reflux, work with your doctor on de-escalation strategies. Many patients can transition to H2 blockers (famotidine) or lifestyle modifications without sacrificing symptom control while causing less microbiome disruption.
The Soil-Based Organism Controversy
There’s emerging interest in soil-based probiotics containing Bacillus species — bacteria common in indigenous guts but rare in Western populations. The theory is these spore-forming bacteria can survive stomach acid and potentially recolonize.
The data is preliminary but intriguing. Studies show Bacillus subtilis and related species can reduce intestinal permeability and modulate immune function. Unlike Lactobacillus probiotics, these may actually establish residence.
But here’s my clinical perspective: we’re essentially trying to reverse-engineer a process that should happen naturally from environmental exposure. It’s better than nothing, but it’s a band-aid on a bullet wound.
The Fecal Transplant Future
Fecal microbiota transplantation (FMT) — transferring complete microbiome communities from healthy donors — is currently FDA-approved only for recurrent C. difficile infections, where it’s 90%+ effective (compared to 25-30% for antibiotics alone).
Researchers are investigating FMT for inflammatory bowel disease, obesity, and metabolic syndrome with mixed results. The challenge is that engraftment depends on the recipient’s existing ecosystem. If your gut environment can’t support diverse bacteria due to low fiber intake, chronic medication use, or other factors, transplanted bacteria won’t establish.
This isn’t ready for prime time outside C. diff, but it represents our growing recognition that microbiome restoration requires entire communities, not individual strains.
What This Means for Your Health Today
Every decision to use antibiotics, PPIs, or NSAIDs should involve a risk-benefit calculation that includes microbiome impact. When I prescribe antibiotics now, I have a different conversation than I did 15 years ago. I explain we’re choosing the lesser evil — treating a dangerous infection — while acknowledging the collateral damage.
The Yanomami and other indigenous populations aren’t healthier across every metric (they have their own health challenges), but their microbiome diversity represents our ancestral baseline. We’ve inadvertently conducted a 100-year experiment on industrialized populations, and the results suggest we’ve impoverished our internal ecosystems in ways that contribute to modern chronic diseases.
The good news: unlike genetic changes, microbiome changes are potentially reversible within your lifetime if we act aggressively. But that requires acknowledging the problem exists, which mainstream medicine has been slow to do.
Your One Action Step
The next time a doctor prescribes an antibiotic, ask three questions: (1) Is this definitely bacterial, not viral? (2) What’s the narrowest-spectrum antibiotic that will work? (3) What’s the consequence of watchful waiting for 48 hours? These questions alone will eliminate a significant portion of unnecessary antibiotic use while protecting your microbiome for genuinely necessary treatments. Your gut bacteria — and your long-term health — will thank you for treating antibiotics as the nuclear option they actually are, not the default they’ve become.


