


The Policy Doesn’t Match The Pharmacology
Even after marijuana’s recent federal reclassification from Schedule I to Schedule III, truck drivers and commercial pilots face an absolute ban on medical cannabis use—even in states where it’s legal, even with a prescription, even if they never use it before work. The Department of Transportation (DOT) hasn’t budged. But mainstream coverage focuses on politics and law while missing the fundamental issue: the human body metabolizes THC in ways that make impairment testing nearly impossible with current technology.
I’m going to explain why this policy exists from a physiological standpoint, not a legal one. Because the real question isn’t whether marijuana should be legal—it’s whether we can accurately measure when someone is actually impaired versus when they simply used cannabis three weeks ago.
THC Metabolism: Why Blood Tests Miss The Point
When you ingest THC (tetrahydrocannabinol), your liver converts it into 11-hydroxy-THC, then into carboxy-THC (THC-COOH), which is fat-soluble and stores in adipose tissue for weeks. Research published in Chemistry & Biodiversity shows THC-COOH can be detected in urine for 30-90 days in regular users, long after any psychoactive effects have worn off.
Here’s the problem: Standard drug tests detect THC-COOH metabolites, not active THC. A positive test means you used marijuana sometime in the past month—it tells you nothing about whether you’re impaired right now. It’s like testing for alcohol by measuring how much you drank last Tuesday.
Blood tests for active THC are better but still flawed. Studies from Clinical Chemistry demonstrate that THC blood levels drop rapidly within 3-4 hours of use, but psychomotor impairment can persist longer in occasional users or disappear faster in chronic users who’ve developed tolerance. There’s no universal blood THC threshold that reliably indicates impairment across all individuals.
The Unique Challenge of Safety-Sensitive Positions
A commercial airline pilot controls 200+ lives. A semi-truck driver operates an 80,000-pound vehicle at highway speeds. The Federal Motor Carrier Safety Administration (FMCSA) and Federal Aviation Administration (FAA) operate under a zero-risk framework for these positions—and they’re not being unreasonable given current technology.
Compare this to alcohol: We have decades of research establishing that a 0.08% blood alcohol concentration (BAC) impairs driving ability in essentially everyone. Breathalyzers measure current blood alcohol accurately. The pharmacokinetics of ethanol are predictable: it’s water-soluble, metabolized at a steady rate (about one drink per hour), and leaves your system completely within 24 hours maximum.
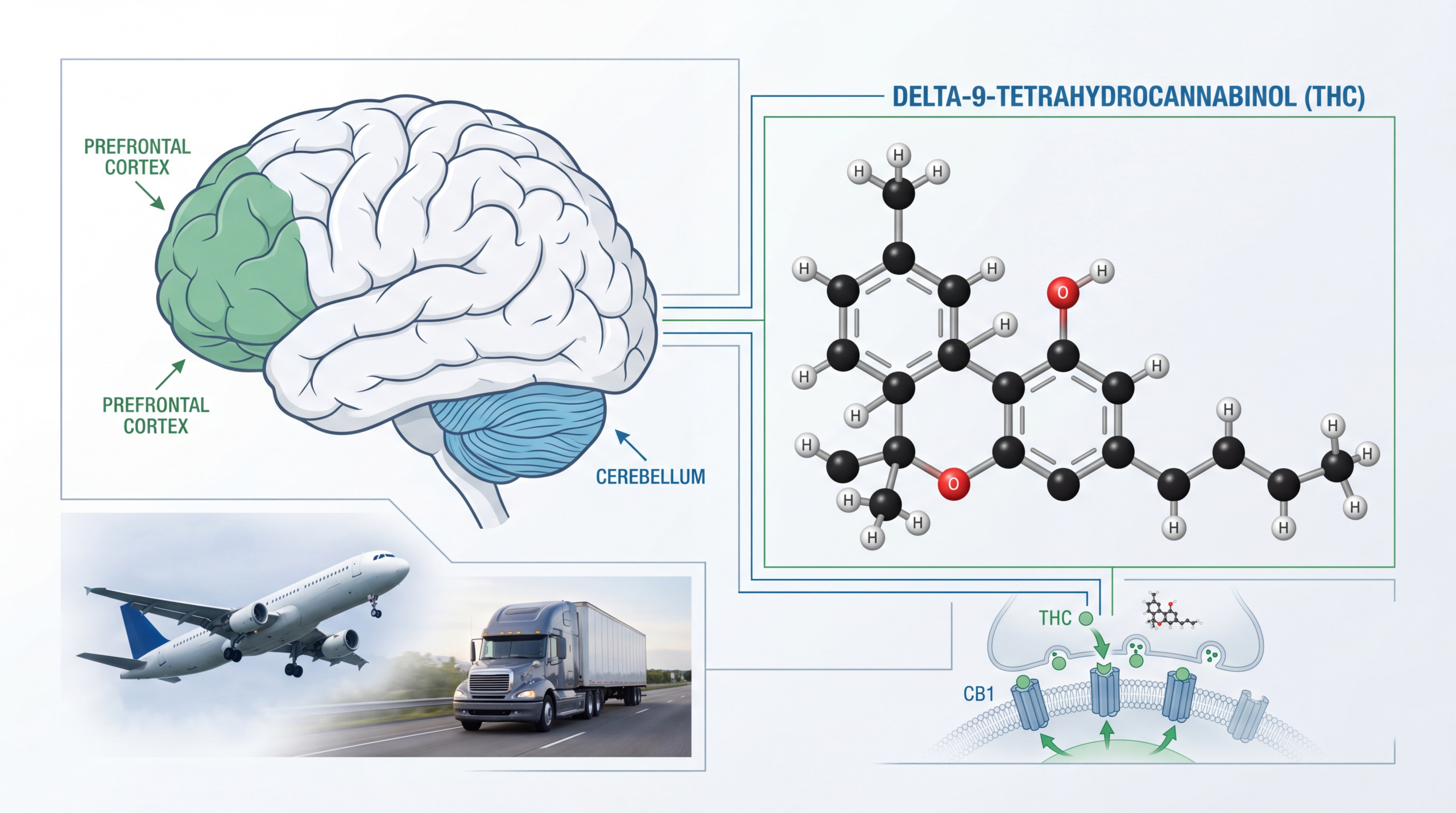
THC doesn’t work that way. Research in the New England Journal of Medicine shows that cannabinoid receptors (CB1 and CB2) are concentrated in brain regions controlling coordination, memory, and time perception—but individual responses vary wildly based on genetics, tolerance, and consumption method (smoking vs. edibles vs. tinctures).
What The Media Consistently Gets Wrong
News coverage treats this as pure political hypocrisy: “Marijuana is medicine now, so why the ban?” That’s intellectually lazy. The issue isn’t whether cannabis has legitimate medical uses—the WHO acknowledges it does. The issue is that we lack a reliable, affordable roadside test for cannabis impairment that works like an alcohol breathalyzer.
Several companies are developing saliva-based tests and breathalyzers for THC, but none have achieved the accuracy and legal acceptance needed for safety-critical industries. A 2020 review in Drug Testing and Analysis found that oral fluid testing shows promise but still can’t distinguish between recent use (2-4 hours ago) and very recent use (30 minutes ago)—a critical distinction when someone is about to fly a plane.
The media also ignores tolerance. A daily cannabis user may show high THC blood levels but perform normally on driving simulators, while an occasional user with lower THC levels shows significant impairment. Research from the Journal of Analytical Toxicology demonstrates this paradox clearly: chronic users develop functional tolerance to many of THC’s impairing effects, but our testing can’t account for that.
The Biological Reality: Cannabinoid Receptor Physiology
Let’s get specific about mechanism. THC binds to CB1 receptors in the cerebellum (motor control), hippocampus (memory formation), and prefrontal cortex (decision-making). When activated, these receptors reduce neurotransmitter release through retrograde signaling—essentially, they tell neurons to “calm down.”
In moderate doses, this can reduce anxiety and pain. In higher doses or in naive users, it impairs reaction time, divided attention, and lane tracking. Meta-analyses in Psychological Bulletin show these effects are dose-dependent and task-dependent: complex tasks requiring sustained attention are impaired more than simple motor tasks.
But here’s what makes this impossibly complex for workplace policy: CB1 receptor density varies between individuals based on genetics and prior cannabis exposure. Someone with naturally lower CB1 expression might experience less impairment at the same THC blood level as someone with higher receptor density. And chronic use downregulates these receptors, creating tolerance—which is why a daily medical user might genuinely be unimpaired at THC levels that would incapacitate an occasional recreational user.
Why the DOT Policy Makes Medical (If Not Political) Sense
The Department of Transportation’s position is this: Until we have a test that accurately measures current impairment—not past use, not blood metabolites, but actual functional impairment—they can’t allow any cannabis use in safety-critical positions. From a public health standpoint, this is defensible.
Consider the alternative: Allow medical marijuana use but rely on self-reporting when drivers or pilots feel impaired. NHTSA data shows that drugged driving fatalities are rising, and cannabis is the most frequently detected non-alcohol substance in fatal crashes. Asking someone to self-assess their own impairment when their prefrontal cortex—the region responsible for judgment—is precisely what’s being affected is circular logic.
The FAA and FMCSA aren’t stupid. They know that many pilots and truckers manage chronic pain, PTSD, and other conditions that cannabis might help. But they also know that one impaired pilot or one truck driver who misjudges stopping distance can kill dozens of people. In risk management, when you can’t measure the risk accurately, you eliminate the exposure entirely.
The Path Forward: Better Testing Technology
The solution isn’t to remove the ban—it’s to develop better testing. Several research groups are working on performance-based impairment testing: cognitive assessments that measure reaction time, divided attention, and decision-making rather than detecting drug metabolites. Studies in Drug and Alcohol Dependence show that these neurocognitive tests correlate better with actual driving impairment than THC blood levels do.
Imagine a system where a pilot or truck driver performs a 5-minute cognitive baseline test when sober, then takes the same test before each shift. If performance drops below their personal baseline by a statistically significant margin, they’re grounded or benched—regardless of what substance (if any) caused the decline. This would catch cannabis impairment, but also catch sleep deprivation, prescription medication side effects, or acute illness.
This technology exists. Companies like Druid and SARA use smartphone-based apps to measure divided attention, balance, and reaction time. The barrier isn’t scientific—it’s regulatory and legal. Courts haven’t yet established these tests as admissible evidence for impairment, and unions reasonably worry about employers using them to unfairly exclude workers.
What About CBD and Other Cannabinoids?
The DOT policy also bans CBD products for pilots and truckers, which seems excessive given that WHO reviews indicate CBD has no abuse potential and doesn’t impair driving. But here’s the catch: The CBD market is poorly regulated. Studies in JAMA found that 69% of CBD products online contained different cannabinoid levels than labeled—including significant THC in products marketed as “THC-free.”
From a policy perspective, the DOT can’t say “CBD is fine as long as it contains zero THC” when the market can’t reliably deliver that promise. A truck driver taking a mislabeled CBD tincture could test positive for THC and legitimately have no idea why. The blanket ban is crude but pragmatic until better product regulation exists.
The Real Victims: Medical Patients Forced to Choose
The people hurt most by this policy are veterans with PTSD, drivers with chronic pain conditions, and pilots with treatment-resistant epilepsy—people for whom cannabis might offer real medical benefit but who must choose between their career and their health.
VA data shows that many veterans use cannabis to manage service-connected disabilities, but if they want to drive commercially, they must rely on opioids instead—which are legal under DOT rules as long as prescribed by a doctor. This creates a perverse incentive: A trucker can take oxycodone daily (which absolutely impairs driving) but can’t use cannabis once on the weekend.
The difference? Opioids are water-soluble and leave your system within 24-48 hours. A driver taking prescription oxycodone at night might test clean the next morning, even if they’re cognitively impaired. Cannabis lingers in fat tissue and tests positive for weeks, even when there’s zero current impairment. The policy punishes the detection window, not the impairment itself.
What Should Actually Happen (But Probably Won’t Soon)
Ideally, federal policy would shift to performance-based impairment testing for all substances. If a pilot can pass a rigorous cognitive test measuring the specific skills needed for safe flight, their cannabinoid metabolite levels shouldn’t matter. If a truck driver demonstrates normal reaction time, attention, and judgment, what they did last weekend is irrelevant.
This would also catch the current problem that DOT drug testing misses: prescription medications that significantly impair driving but aren’t tested for. Benzodiazepines, muscle relaxants, and sedating antihistamines all impair driving more than residual cannabis from last week—but only cannabis triggers a positive test.
The Mayo Clinic notes that opioid medications affect reaction time and decision-making, yet they’re permitted in safety-sensitive positions as long as a doctor prescribed them. The inconsistency isn’t about safety—it’s about what we can test for reliably.
What You Should Actually Do
If you’re a pilot or commercial driver considering medical cannabis: Don’t. Not because it won’t help your condition, but because one positive test ends your career permanently. The DOT maintains a national database of failed drug tests, and you cannot get a safety-sensitive transportation job after a verified positive result—even decades later.
If you’re managing chronic pain, work with a physician who understands non-opioid alternatives that won’t trigger DOT testing: physical therapy, non-sedating muscle relaxants, targeted injections, or neuromodulation techniques. NIH-funded studies show that acupuncture, cognitive behavioral therapy, and exercise programs can match cannabis’s pain relief without the career-ending test results.
If you’re a policymaker: Fund research into performance-based impairment testing and push for federal standards that measure function, not metabolites. The current system is simultaneously too harsh (banning weekend cannabis use that causes zero Monday impairment) and too lenient (allowing impairing prescription medications because they clear quickly).
The Bottom Line
The DOT ban on medical marijuana for pilots and truckers isn’t political theater—it’s an admission that our drug testing technology is stuck in the 1980s. We can’t measure cannabis impairment accurately, so we ban it entirely in high-stakes jobs where error costs lives.
That’s not satisfying, but it’s honest. The real fight should be for better testing methods that measure what actually matters: whether you’re safe to fly a plane or drive a truck right now, regardless of what you consumed last week.
Until we can measure impairment instead of metabolites, safety-critical workers will keep choosing between their health and their careers—and that’s the biological reality the reclassification can’t change.


