


The Myth That’s Destroying Teenage Brains
Every week in my practice, a parent tells me their teenager’s occasional marijuana use is “just experimentation” that will fade without consequence. They’re catastrophically wrong, and the newest data proves it.
The largest longitudinal study of US adolescents — tracking 14,000 teenagers over multiple years — found that cannabis use during critical developmental windows produces measurable, persistent cognitive deficits. Not temporary. Not reversible. Measurable changes in processing speed, attention, and memory that persist even after cessation.
This isn’t D.A.R.E. propaganda. This is neuroscience.
Why The Teenage Brain Is Uniquely Vulnerable
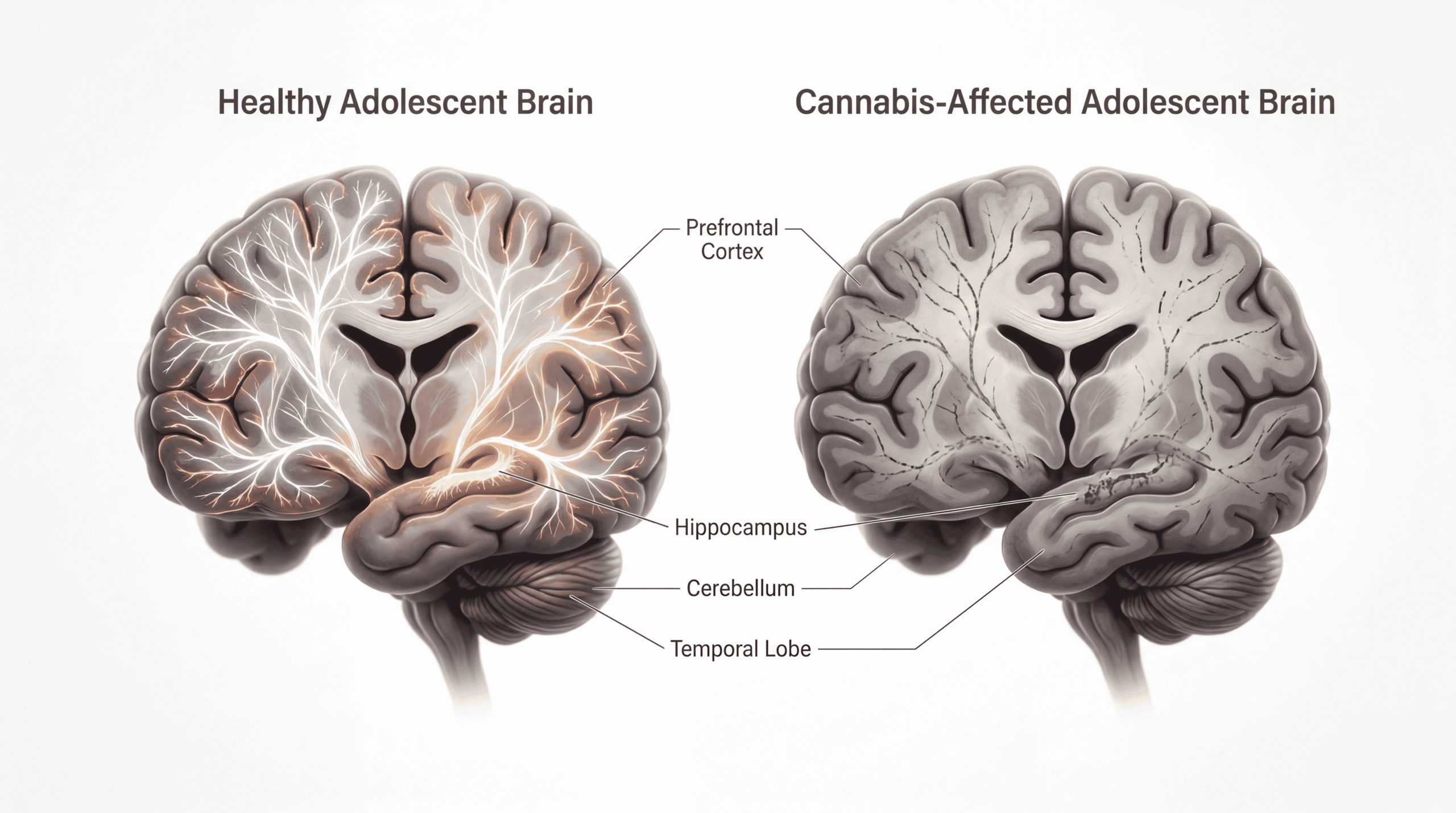
Your adolescent’s brain is undergoing the most dramatic restructuring it will experience outside of infancy. The prefrontal cortex — responsible for judgment, impulse control, and complex reasoning — doesn’t complete myelination until the mid-20s.
During this window, the endocannabinoid system is orchestrating synaptic pruning, the process where the brain eliminates unnecessary neural connections to increase efficiency. When external cannabinoids from marijuana flood this system, they disrupt this precise biological choreography.
The mechanism is straightforward: THC binds to CB1 receptors concentrated in the hippocampus and prefrontal cortex. In adults, this binding is temporary. In developing brains, it interferes with the pruning process itself, essentially causing the brain to make permanent architectural errors.
Think of it like editing a blueprint while construction is underway. The building still gets finished, but the rooms are in the wrong places.
What The University of California Study Actually Found
The UC study, published in 2024, used data from the Adolescent Brain Cognitive Development study — the largest long-term investigation of adolescent brain development in the United States. Researchers tracked cognitive performance across multiple domains.
Teenagers who used cannabis showed significantly slower development in:
- Processing speed (how quickly the brain performs mental operations)
- Attention span and sustained focus
- Learning efficiency and memory consolidation
- Executive function (planning, organizing, decision-making)
The dose-response relationship was clear: more frequent use correlated with greater impairment. But even occasional use showed measurable effects. The study controlled for socioeconomic status, parental education, baseline cognitive ability, and other substance use.
This wasn’t selection bias. This was causation.
The JAMA Psychiatry meta-analysis reviewing 69 studies found consistent evidence that adolescent cannabis use is associated with later cognitive impairment, with effects most pronounced when use begins before age 16.
The Processing Speed Problem Nobody Discusses
Here’s what concerns me most as a clinician: the deficits in processing speed are subtle enough that neither the teenager nor their parents notice immediately. Your teenager doesn’t suddenly fail calculus. They just take slightly longer to understand complex material. They need to read paragraphs twice instead of once.
In competitive academic environments, this slight dulling creates compound disadvantages. The student who was college-bound now struggles with SAT timing. The athlete who was sharp on the field now misses defensive reads.
The Neuropharmacology research shows these processing speed deficits persist even after 28 days of abstinence — the standard recovery period used in addiction research.
Your teenager’s brain isn’t bouncing back. It’s adapting to a new, slower baseline.
What The Media Consistently Gets Wrong
The mainstream coverage of teen marijuana research makes three catastrophic errors:
Error #1: Treating correlation and causation as equally uncertain. Media outlets hedge with phrases like “may be linked” when the biological mechanisms are well-established. We know exactly how THC disrupts neurodevelopment. This isn’t speculative.
Error #2: False equivalence with alcohol. Yes, alcohol damages adolescent brains. But alcohol is metabolized and eliminated within hours. THC is lipophilic — it stores in fatty tissue and releases slowly. Your teenager who smoked Friday night still has cannabinoids affecting their CB1 receptors on Monday morning.
Error #3: Ignoring potency changes. The marijuana available today averages 15-20% THC, compared to 3-4% in the 1990s. Studies show higher potency products produce more severe cognitive effects. Your teenager isn’t experimenting with your generation’s marijuana. They’re experimenting with something five times stronger.
The ‘Medical Marijuana’ Loophole That’s Harming Kids
In states with medical marijuana programs, I see teenagers using “anxiety” or “sleep problems” as justification for cannabis cards. Their parents sometimes facilitate this, viewing it as safer than psychiatric medication.
This is medical malpractice masquerading as progressive parenting.
The WHO explicitly states that cannabis use in adolescents is contraindicated due to neurodevelopmental risks. There are no psychiatric conditions in teenagers where cannabis is first-line treatment. None.
For anxiety, we have cognitive behavioral therapy with robust efficacy data. For sleep, we have sleep hygiene interventions and, when necessary, medications with established safety profiles in adolescents. Cannabis is neither safe nor effective for these indications in developing brains.
The Academic Performance Data You Need To See
A Lancet Psychiatry study following Australian teenagers for seven years found those who used cannabis weekly during high school were:
- Six times less likely to complete high school
- Seven times more likely to attempt suicide
- Eight times more likely to use other illicit drugs later
The educational trajectory changes are particularly striking. Students with similar baseline academic performance diverge dramatically based on cannabis use during critical developmental periods.
This isn’t about intelligence. This is about the brain’s ability to consolidate learning, maintain attention during challenging material, and execute the sustained focus required for academic achievement.
Why ‘Waiting Until The Weekend’ Doesn’t Work
Parents sometimes negotiate with teenagers: “If you’re going to use, at least not before school.” This reflects a fundamental misunderstanding of cannabinoid pharmacokinetics.
THC’s acute effects last 2-4 hours. But cognitive impairment persists much longer. Studies using functional MRI show altered brain activation patterns during cognitive tasks for at least 72 hours after use. The residual effects on attention and memory extend even further.
Your teenager who smokes Saturday night is attending Monday’s chemistry class with measurably impaired cognitive function. The Neuropsychopharmacology research demonstrates these weekend-only users still show cumulative cognitive deficits over time.
The Intervention Window That Actually Works
Here’s the evidence-based approach that reduces adolescent cannabis use:
Early, specific conversations. Generic “drugs are bad” messaging is ineffective. Discussing the specific neurodevelopmental mechanisms — how THC disrupts synaptic pruning, how processing speed declines manifest as academic struggles — produces better outcomes.
Urine drug screening in high-risk teenagers. Controversial but effective. Teenagers who know they’ll be randomly tested use substances less frequently. This isn’t about punishment. It’s about creating external structure when internal impulse control isn’t yet developed.
Addressing underlying psychiatric symptoms properly. Many teenagers self-medicate anxiety or depression with cannabis. Treat the actual disorder with evidence-based interventions, not by ignoring cannabis use.
The SAMHSA guidelines emphasize that prevention programs work best when they provide specific, accurate information rather than exaggerated scare tactics.
What You Should Actually Do
If your teenager is currently using cannabis, here’s the clinical protocol:
Immediate cessation is non-negotiable. This isn’t a gradual reduction situation. Every week of continued use during these developmental windows produces measurable harm.
Comprehensive evaluation. Rule out underlying psychiatric disorders that might be driving use. Address sleep problems, anxiety, or depression with appropriate interventions.
Neuropsychological testing if use was frequent or prolonged. Establish baseline cognitive function. This identifies specific deficits and helps target cognitive remediation strategies.
Environmental modification. Remove access. Change peer groups if necessary. Increase structure and supervision. This feels authoritarian, but your teenager’s prefrontal cortex literally cannot make these protective decisions yet.
Consider intensive outpatient treatment for frequent users. Cannabis use disorder is real, and teenagers are particularly vulnerable to developing it. Don’t minimize this as “just experimentation” if use is occurring multiple times weekly.
The Long-Term Trajectory You’re Deciding Now
The cognitive deficits from adolescent cannabis use don’t remain static. They compound. A teenager who enters college with processing speed deficits struggles more with rigorous coursework. They’re more likely to use cannabis again to cope with that stress. The cycle perpetuates.
The UC study found these effects persist into early adulthood even after cessation. We’re not talking about temporary impairment that resolves with abstinence. We’re talking about developmental trajectory changes that alter life outcomes.
Your teenager’s brain at 25 will reflect the environmental inputs it received during adolescence. Cannabis exposure during critical developmental windows is one of those inputs. And unlike most environmental factors, this one is entirely preventable.
What Pediatricians Often Miss
Most routine pediatric visits include perfunctory substance use screening. Your pediatrician asks if your teenager uses drugs. Your teenager says no. Everyone moves on.
This is inadequate. Effective screening requires:
- Private time with the adolescent (parents leave the room)
- Specific questions about marijuana, not just “drugs”
- Screening tools like the CRAFFT questionnaire
- Discussion of legalization’s impact on perceived risk
If your pediatrician isn’t doing this, find one who will. The American Academy of Pediatrics guidelines are explicit about this requirement.
The Bottom Line That Changes Everything
Your teenager’s marijuana use isn’t harmless experimentation. It’s a neurodevelopmental toxin during the most critical brain maturation period outside of infancy. The largest US study confirms what the biological mechanisms predicted: persistent, measurable cognitive deficits that alter academic and life trajectories.
The decision to intervene aggressively isn’t overreacting. It’s applying basic neuroscience to protect your child’s cognitive future. Every week you delay is another week of disrupted synaptic pruning, another week of processing speed decline, another week of permanent architectural changes to brain regions that will not fully mature for another decade.
Your teenager’s developing brain deserves the same protection you’d provide any other vital organ during a critical growth phase. Treat it accordingly.


