


The weight loss drug revolution isn’t about willpower anymore—it’s about a hormone most people have never heard of, and it’s already outperforming the medications making headlines.
While everyone’s talking about Ozempic and Wegovy (semaglutide), the real breakthrough is happening with glucose-dependent insulinotropic polypeptide, or GIP. This gut hormone, working alongside its more famous cousin GLP-1, is showing weight loss results that frankly surprised even researchers like me who’ve spent decades studying metabolic disease.
What GIP Actually Does (And Why It Matters More Than You Think)
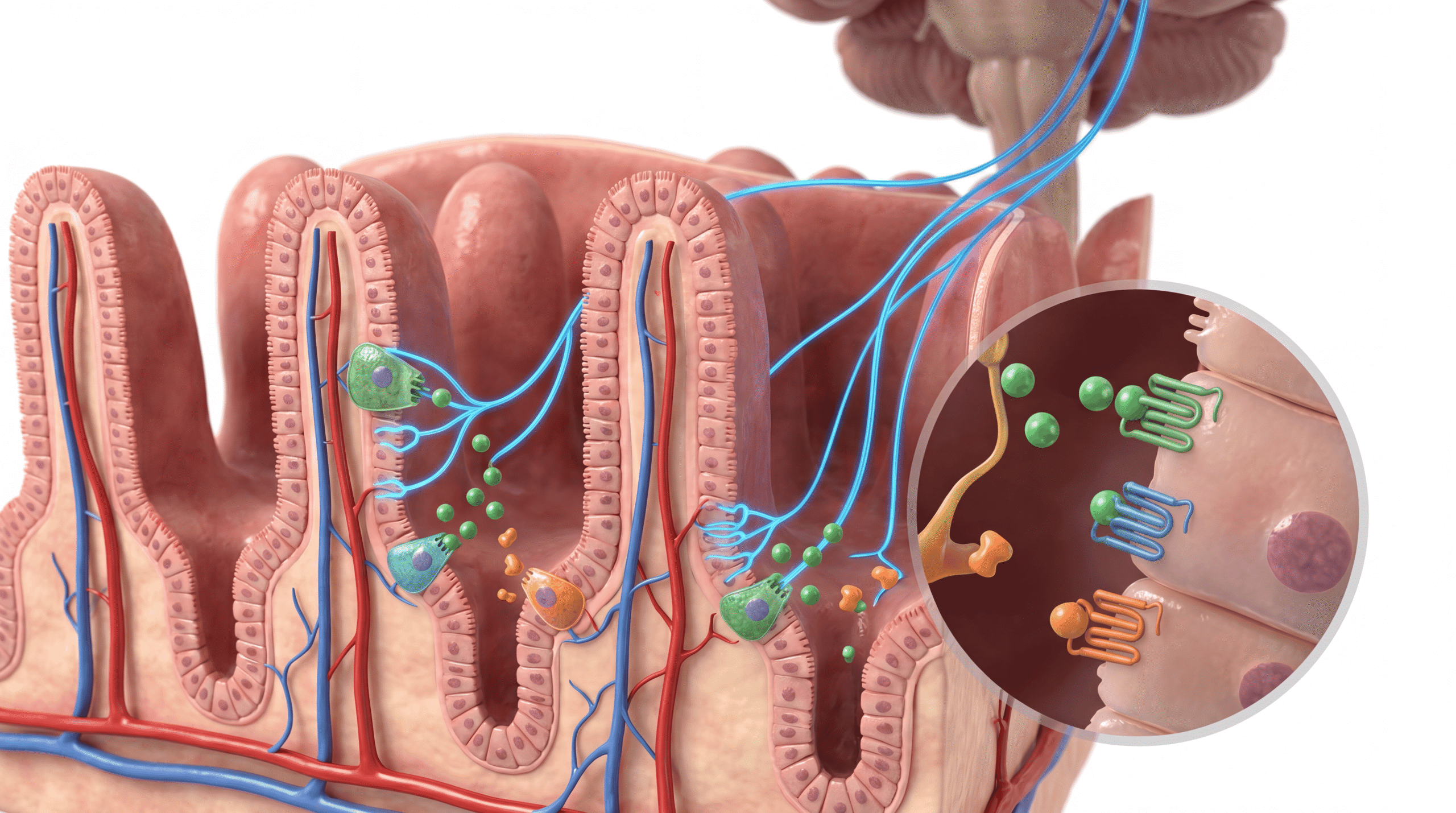
GIP is an incretin hormone—a signaling molecule released by your small intestine within minutes of eating. For years, we thought its primary job was stimulating insulin release when blood sugar rises. That’s partially true, but we massively underestimated its role in energy metabolism and fat storage.
Here’s the mechanism that changes everything: GIP binds to receptors not just in your pancreas, but throughout your adipose tissue, brain, and even bone. When activated in fat cells, GIP receptors trigger a cascade that enhances insulin sensitivity and promotes fat storage in a controlled, metabolically healthy way—preventing the dangerous ectopic fat accumulation in your liver and muscles that drives type 2 diabetes.
But the real revelation came when researchers started blocking GIP receptors in animal models. They expected improved glucose control. Instead, they got dramatic weight loss. The animals ate less, burned more energy, and their fat cells literally shrank.
Why Tirzepatide Is Destroying the Competition
Tirzepatide (brand name Mounjaro for diabetes, Zepbound for weight loss) is the first dual GIP/GLP-1 receptor agonist approved for clinical use. In the SURMOUNT-1 trial published in the New England Journal of Medicine, patients lost an average of 22.5% of their body weight at the highest dose—that’s not a typo.
Compare that to semaglutide’s 15% average weight loss, and you see why pharmaceutical companies are scrambling to develop GIP-based therapies. The difference isn’t marginal—it’s clinically transformative for patients who’ve struggled with obesity for decades.
The mechanism behind tirzepatide’s superiority involves complementary pathways. GLP-1 receptor activation suppresses appetite through brainstem and hypothalamic signaling, slows gastric emptying, and reduces glucagon secretion. GIP receptor activation appears to enhance these effects while simultaneously improving insulin sensitivity and potentially increasing energy expenditure through brown adipose tissue activation.
The Part That Challenges Everything We Thought We Knew
Here’s where it gets controversial: For years, researchers assumed that blocking GIP receptors would be therapeutic for obesity and diabetes. The logic seemed sound—GIP promotes insulin release and theoretically could worsen insulin resistance. Some pharmaceutical companies spent millions developing GIP receptor antagonists.
They were completely wrong. The dual agonist approach—activating both GIP and GLP-1 receptors simultaneously—produces synergistic effects that neither hormone achieves alone. We still don’t fully understand why, but the clinical data is undeniable.
One hypothesis involves GIP’s complex effects on adipocyte biology. At physiological doses, GIP may actually improve the metabolic health of existing fat tissue while the GLP-1 component reduces overall food intake. The result: you lose weight while simultaneously improving the function of remaining adipose tissue—a metabolic win-win we’ve never achieved with previous obesity medications.
What The Media Got Wrong
The mainstream coverage of these medications has been embarrassingly superficial. Headlines focus on celebrities using “diabetes drugs” for weight loss, completely missing the underlying science and the legitimate medical revolution happening.
First, calling tirzepatide just a “diabetes drug” is like calling penicillin just a “syphilis treatment.” Yes, it treats diabetes brilliantly (HbA1c reductions exceeding 2%), but it’s fundamentally an obesity medication that happens to also treat the metabolic dysfunction underlying type 2 diabetes. The disease model itself has shifted—we now understand that obesity is the primary pathology, and diabetes is often a downstream consequence.
Second, the media completely ignores the mechanistic differences between medications. They treat all GLP-1 drugs as interchangeable when the addition of GIP receptor activation represents a genuine pharmacological leap forward, not just incremental improvement.
Third, the safety concerns are overblown and misdirected. Yes, these medications cause nausea in some patients, especially during dose titration. Yes, there are rare cases of pancreatitis. But the absolute risk is tiny compared to the cardiovascular and metabolic devastation of untreated obesity. We’re talking about medications that reduce major adverse cardiovascular events by 20-26% in high-risk patients—that’s comparable to statin therapy.
The Biological Reality of GIP That Changes Patient Outcomes
Understanding GIP’s physiology explains why these drugs work when everything else failed for so many patients. Your body releases GIP in response to nutrient intake, particularly fats and carbohydrates. In people with obesity, GIP signaling often becomes dysregulated—higher baseline levels but blunted responses to meals, contributing to the metabolic inflexibility that makes weight loss nearly impossible through diet alone.
Pharmaceutical GIP receptor agonists restore and amplify this signaling in a sustained, pharmacological manner that diet simply cannot replicate. You’re not fighting your biology anymore—you’re working with it at a molecular level. The hypothalamic circuits that drive hunger, the gastric motility that affects satiety, the pancreatic beta cells that regulate glucose—they’re all responding to signals your body recognizes as natural, just at therapeutic intensities.
This is why patients on tirzepatide consistently report that food noise quiets. They’re not whiteknuckling through hunger—their appetite physiology has fundamentally changed. The compulsive food thoughts, the constant hunger between meals, the inability to feel satisfied—these aren’t character flaws, they’re hormonal dysregulation, and GIP/GLP-1 agonists directly address the underlying pathology.
What’s Coming Next (And It’s Not What You Expect)
The next generation isn’t just about dual agonists—it’s about triple agonists. Retatrutide, currently in Phase 3 trials, adds glucagon receptor activation to the GIP/GLP-1 combination. Early data shows average weight loss approaching 24% at 48 weeks, with some patients losing more than 30% of their body weight.
The addition of glucagon receptor activation increases energy expenditure and promotes lipolysis—your body literally burns stored fat more efficiently. We’re approaching weight loss magnitudes previously only achievable through bariatric surgery, but with a weekly injection instead of permanently altering your anatomy.
But here’s what really excites me as a physician: These medications are changing outcomes beyond weight. The SELECT cardiovascular outcomes trial demonstrated that semaglutide reduces cardiovascular events regardless of initial weight loss magnitude, suggesting direct cardiovascular effects independent of weight reduction. Tirzepatide trials are showing improvements in liver steatosis, sleep apnea, and inflammatory markers.
We’re not just treating obesity anymore—we’re treating the systemic metabolic dysfunction that obesity reflects. That’s a paradigm shift in how we approach chronic disease.
The Resistance You’ll Face (And Why It’s Misguided)
Despite overwhelming evidence, you’ll still encounter physicians who view these medications as “cheating” or who insist patients should “try diet and exercise first.” This is medical paternalism rooted in outdated understanding of obesity pathophysiology.
Obesity is not a willpower disorder—it’s a complex neuroendocrine disease involving dozens of hormones, neuropeptides, and metabolic feedback loops. Expecting diet and exercise alone to overcome leptin resistance, ghrelin dysregulation, and reduced metabolic rate is like expecting a type 1 diabetic to produce insulin through positive thinking.
The data is clear: Fewer than 5% of people with obesity achieve sustained weight loss (defined as losing ≥10% of body weight and maintaining it for 5+ years) through lifestyle modification alone. Not because they’re weak or uncommitted, but because the biological mechanisms defending elevated body weight are stronger than conscious effort can overcome.
What You Should Actually Do
If you’re struggling with obesity (BMI ≥30) or overweight with metabolic complications (BMI ≥27 with type 2 diabetes, hypertension, or dyslipidemia), have an honest conversation with your physician about GIP/GLP-1 therapy. Not as a last resort after years of failed dieting, but as a first-line treatment for a chronic disease.
Understand that these medications work best as part of comprehensive care—you still need adequate protein intake to preserve lean mass during weight loss, resistance training to maintain muscle, and behavioral strategies to build sustainable eating patterns. But you’re not doing it with your metabolism actively fighting you at every step.
If cost is a barrier—and it absolutely is for many patients, with list prices exceeding $1,000 monthly—be aggressive about prior authorization, manufacturer savings programs, and honestly, raising hell about insurance coverage. These medications prevent heart attacks, strokes, and diabetic complications. Covering them is cost-effective from any rational healthcare economics perspective.
For patients already on semaglutide or liraglutide with suboptimal response, switching to tirzepatide is worth discussing. The additional GIP receptor activation may provide the extra metabolic push needed for meaningful outcomes. Don’t accept “good enough” when better options exist.
The Bottom Line That Actually Matters
GIP isn’t just another incretin hormone—it’s the mechanistic explanation for why dual agonist therapy represents genuine innovation in obesity pharmacology. The combination of GIP and GLP-1 receptor activation addresses multiple pathological pathways simultaneously, producing weight loss that finally matches the magnitude of the problem.
We’re living through a revolution in how we treat metabolic disease. The medications work, the safety profile is acceptable, and the outcomes transform lives. The only remaining barriers are cost, access, and outdated attitudes about obesity that belong in the 20th century, not modern medicine.
You deserve treatment that addresses the biology driving your disease, not lectures about willpower that ignore everything we’ve learned about metabolic physiology in the past two decades.


